

Journal of Clinical Pediatrics ›› 2025, Vol. 43 ›› Issue (10): 775-781.doi: 10.12372/jcp.2025.24e1306
• Clinical Report • Previous Articles Next Articles
ZHENG Ruixue, SUN Xiaodong, WU Guilan, SHEN Leilei( )
)
Received:2024-12-05
Accepted:2025-05-26
Published:2025-10-15
Online:2025-09-29
CLC Number:
ZHENG Ruixue, SUN Xiaodong, WU Guilan, SHEN Leilei. Neonatal refractory congenital chylothorax: two case reports and literature review[J].Journal of Clinical Pediatrics, 2025, 43(10): 775-781.

Figure 1
Changes in chest X-ray of Case 1 before and after treatment with propranolol"
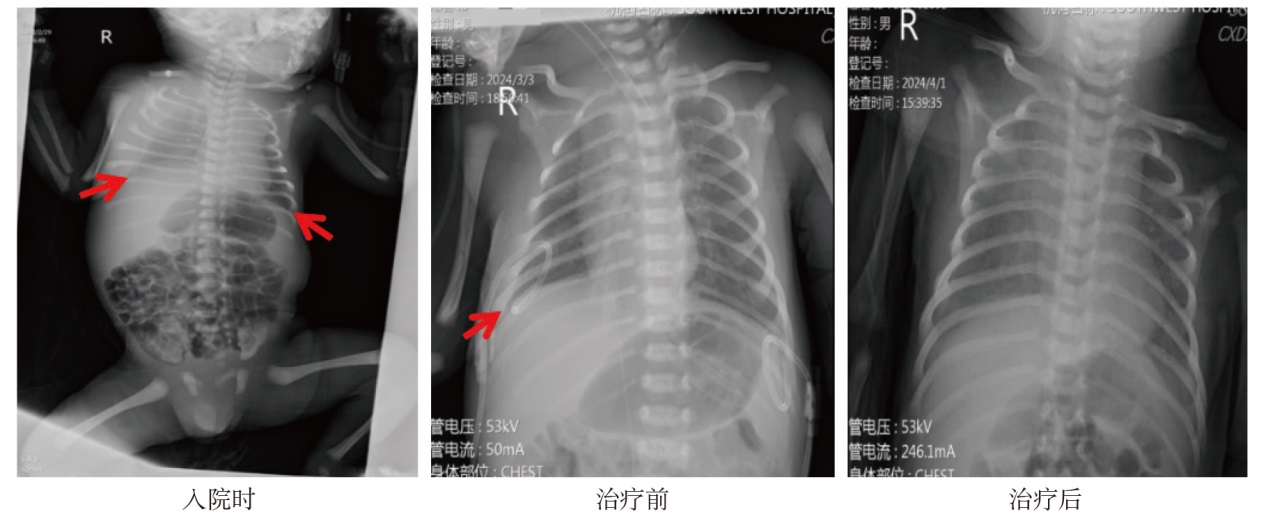
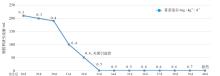
Figure 2
Dynamic changes in thoracostomy drainage and propranolol medication"
Figure 3
The imaging changes of propranolol before and after treatment in Case 2"
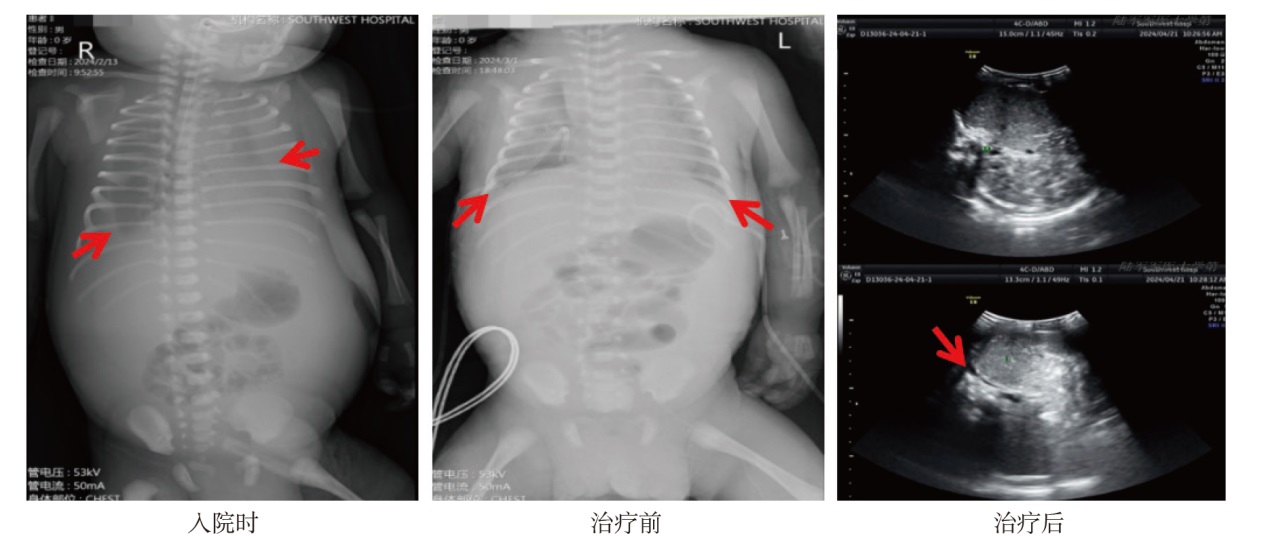

Figure 4
Dynamic changes in pleural effusion volume and propranolol medication"
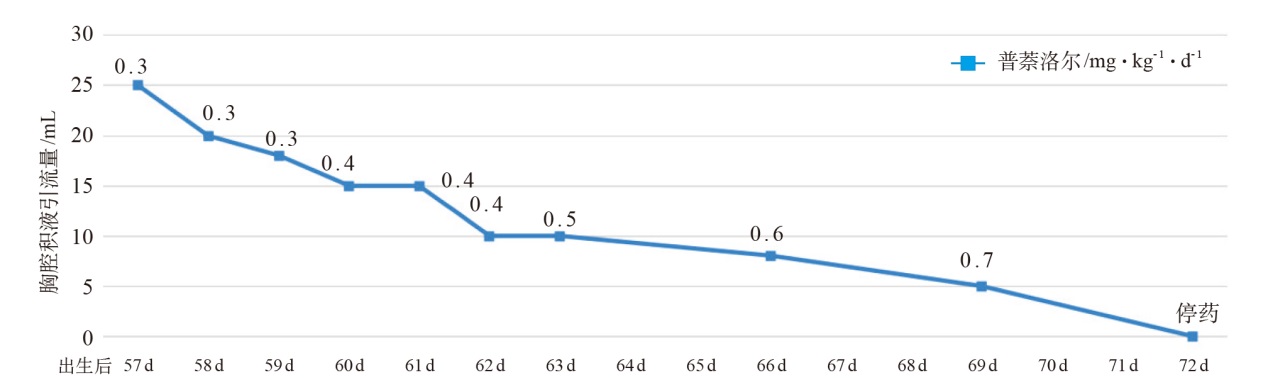
Table 1
General status and treatment outcomes of 30 cases of refractory CC"
| 编号 | 性别 | 出生胎龄/ 周 | 体重/g | 产前是否诊断 胸腔/腹腔积液 | Apgar评分 | 治疗与结局 | |
|---|---|---|---|---|---|---|---|
| 1min | 5min | ||||||
| 患儿1 | 男 | 36 | 3 100 | 是 | 7 | 8 | 治愈,口服普萘洛尔 |
| 患儿2 | 男 | 35+3 | 3 460 | 是 | 6 | 8 | 治愈,口服普萘洛尔 |
| 3[ | — | 34+1 | 2 047 | 是 | 1 | 3 | 治愈,口服依替福林 |
| 4[ | — | 36 | 5 275 | 是 | 4 | 7 | 治愈,口服米多君 |
| 5[ | 女 | 33+6 | — | 否 | — | — | 治愈,大剂量奥曲肽(30.0μg·kg-1·h-1) |
| 6[ | 男 | 37+4 | 3 155 | 是 | 6 | 10 | 治愈,大剂量奥曲肽(20.0μg·kg-1·h-1) |
| 7[ | 女 | 36 | 2 700 | 是 | — | — | 治愈,化学胸膜固定术(胸腔内注射聚维酮碘) |
| 8[ | 男 | 足月 | 3 290 | 否 | — | — | 治愈,胸膜穿刺 |
| 9[ | 女 | 足月 | 2 700 | 否 | — | — | 治愈,胸膜穿刺 |
| 10[ | 男 | 36 | 3 020 | 否 | — | — | 治愈,胸膜穿刺 |
| 11[ | 男 | 36 | 3 000 | 否 | — | — | 死亡(败血症),胸膜穿刺 |
| 12[ | 男 | 35+2 | 3 040 | 是 | 7 | 8 | 死亡,胸腔镜下探查术 |
| 13[ | 女 | 31 | — | 是 | — | — | 治愈,化学胸膜固定术(胸腔内注射聚维酮碘) |
| 14[ | 女 | 35 | 2 300 | 是 | — | — | 治愈,化学胸膜固定术(胸腔内注射聚维酮碘) |
| 15[ | — | 36 | — | — | — | — | 治愈,化学胸膜固定术(胸腔内注射聚维酮碘) |
| 16[ | — | 36 | — | 是 | — | — | 死亡(肾衰竭),化学胸膜固定术(胸腔内注射聚维酮碘) |
| 17[ | 男 | 37 | 3 000 | 是 | 8 | 9 | 治愈,注射索马托司他丁 |
| 18[ | 女 | 33 | 2 510 | 是 | 7 | 9 | 治愈,注射索马托司他丁 |
| 19[ | 男 | 40 | 4 160 | 是 | 9 | 10 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 20[ | 女 | 33 | 2 430 | 是 | 6 | 8 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 21[ | 男 | 31 | 2 320 | 是 | 5 | 8 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 22[ | 女 | 35 | 2 250 | 否 | 9 | 9 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 23[ | 女 | 38 | 3 430 | 是 | 9 | 10 | 死亡(因其他疾病),化学胸膜固定术(胸腔内注射红霉素) |
| 24[ | 男 | 39 | 3 750 | 否 | 10 | 10 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 25[ | 男 | 40 | 3 400 | 否 | 10 | 10 | 失访(因可疑食管气管瘘),化学胸膜固定术(胸腔内注射红霉素) |
| 26[ | 女 | 37 | 3 570 | 否 | 10 | 10 | 治愈,淋巴管瘘修补术 |
| 27[ | 男 | 40 | 3 320 | 否 | 10 | 10 | 治愈,淋巴管瘘修补术 |
| 28[ | 女 | 38 | 3 350 | 否 | 10 | 10 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 29[ | 男 | 39 | 2 990 | 否 | 10 | 10 | 治愈,化学胸膜固定术(胸腔内注射红霉素) |
| 30[ | 女 | 36+5 | 3 281 | 是 | 1 | 8 | 治愈,口服西地那非 |
| [1] | Resch B, Sever Yildiz G, Reiterer F. Congenital chylothorax of the newborn: a systematic analysis of published cases between 1990 and 2018[J]. Respiration, 2022, 101(1): 84-96. |
| [2] |
Attar MA, Donn SM. Congenital chylothorax[J]. Semin Fetal Neonatal Med., 2017, 22(4): 234-239.
doi: S1744-165X(17)30040-9 pmid: 28351595 |
| [3] | Bellini C, Boccardo F, Bellini T. Congenital chylothorax of the newborn[J]. Respiration, 2022, 101(8): 793-794. |
| [4] | Shao XM, Ye HM, Qiu XS. Practical neonatology[M]. People's Medical Publishing House, 2011. |
| [5] | Kasdallah N, Kbaier H, Salem B, et al. Povidone iodine pleurodesis for refractory congenital chylothorax: a review of literature[J]. Tunis Med, 2016, 94(12): 834. |
| [6] | Tomobe Y, Mizuguchi U, Shimotakahara A, et al. Combination therapy with etilefrine and pleurodesis for refractory congenital chylothorax[J]. Biomedicine hub, 2020, 5(3): 1-5. |
| [7] | Tamaoka S, Osada A, Kin T, et al. Midodrine, an oral alpha-1 adrenoreceptor agonist, successfully treated refractory congenital chylous pleural effusion and ascites in a neonate[J]. Chest, 2021, 159(4): e189-e191. |
| [8] | Sahoo T, Mangla MK, Sethi A, et al. Successful treatment of congenital chylothorax with skimmed milk and long course octreotide[J]. BMJ Case Reports CP, 2018, 11(1): bcr-2018-226347. |
| [9] | Vass G, Evans Fry R, Roehr CC. Should newborns with refractory chylothorax be tried on higher dose of octreotide?[J]. Neonatology, 2021, 118(1): 122-126. |
| [10] | Hmami F, Oulmaati A, Bouchikhi C, et al. Congenital chylothorax: rapid and complete response to polyvidone iodine[J]. Arch Pediatr, 2014, 21(9): 1002-1005. |
| [11] |
Altuncu E, Akman İ, Kiyan G, et al. Report of three cases: congenital chylothorax and treatment modalities[J]. Turk J Pediatr, 2007, 49(4): 418-421.
pmid: 18246745 |
| [12] |
Salem P. A neonate with bilateral refractory chylothorax[J]. Med J Malaysia, 1991, 46(4): 376-378.
pmid: 1840449 |
| [13] | Lyu M, Liao ZC, Yu XH, et al. Fetal pleural effusion in the uterus and dyspnea after birth[J]. Zhongguo Dangdai Erke Zazhi, 2020, 22(8): 892-896. |
| [14] | Brissaud O, Desfrere L, Mohsen R, et al. Congenital idiopathic chylothorax in neonates: chemical pleurodesis with povidone-iodine (Betadine)[J]. Arch Dis Child Fetal Neonatal Ed, 2003, 88(6): F531-F533. |
| [15] | González Santacruz M, Tarazona Fargueta JL, Muñoz Alvarez P, et al. Use of somatostatin in five neonates with chylothorax[J]. An Pediatr (Barc), 2005, 63(3): 244-248. |
| [16] | 华敏敏, 夏磊, 霍婉莹, 等. 新生儿先天性乳糜胸的临床及预后影响因素分析[J]. 临床儿科杂志, 2023, 41(1): 25-29. |
| Hua MM, Xia Lei, Huo WY, et al. Analysis of clinical and prognostic factors of neonatal congenital chylothorax[J]. Linchuang Erke Zazhi, 2023, 41(1): 25-29. | |
| [17] |
Malleske DT, Yoder BA. Congenital chylothorax treated with oral sildenafil: a case report and review of the literature[J]. J Perinatol, 2015, 35(5): 384-386.
doi: 10.1038/jp.2015.10 pmid: 25917021 |
| [18] | Yang C, Peng J, Chi J, et al. Comparison of the clinical characteristics of congenital chylothorax in preterm and term infants[J]. Chinese Journal of Neonatology, 2021: 12-16. |
| [19] |
Itkin M, Chidekel A, Ryan KA, et al. Abnormal pulmonary lymphatic flow in patients with paediatric pulmonary lymphatic disorders: diagnosis and treatment[J]. Paediatr Respir Rev, 2020, 36: 15-24.
doi: 10.1016/j.prrv.2020.07.001 pmid: 32792289 |
| [20] | 王斯瑶, 李娟. 新生儿淋巴管发育异常研究进展[J]. 国际儿科学杂志, 2019, 46(1): 48-52. |
| Wang SY, Li J. Research progress on neonatal lymphatic dysplasia[J]. Guoji Erkexue Zazhi, 2019, 46 (1): 48-52. | |
| [21] | Pérez-Pérez A, Vigil-Vázquez S, Gutiérrez-Vélez A, et al. Chylothorax in newborns after cardiac surgery: a rare complication?[J]. Eur J Pediatr, 2023, 182(4): 1569-1578. |
| [22] | Kambara M, Ibara S. Chylothorax as a complication of congenital myotonic dystrophy: a retrospective cohort study[J]. Early Hum Dev, 2021, 158: 105396. |
| [23] | Ball PL, Nethercott S, Beardsall K. Rare case of congenital chylothorax and challenges in its management[J]. BMJ Case Rep, 2019, 12(5): e228023. |
| [24] | Takahashi Y, Kinoshita Y, Kobayashi T, et al. Management of refractory chylothorax in the neonatal intensive care unit: a 22‐year experience[J]. Pediatr Int, 2022, 64(1): e15043. |
| [25] |
Wang B, Feng Y, Guo Y, et al. Clinical features and outcomes of congenital chylothorax: a single tertiary medical center experience in China[J]. J Cardiothorac Surg, 2022, 17(1): 276.
doi: 10.1186/s13019-022-02009-z pmid: 36303149 |
| [26] |
Marino LV, Bell KL, Woodgate J, et al. An international survey of the nutrition management of chylothorax: a time for change[J]. Cardiol Young, 2019, 29(9): 1127-1136.
doi: 10.1017/S1047951119001525 pmid: 31414980 |
| [27] | Kobeisy SAN, Alkhotani A, Barzanji MM. Octreotide infusion for the treatment of congenital chylothorax[J]. Case Rep Pediatr, 2020, 2020(1): 8890860. |
| [28] |
Church JT, Antunez AG, Dean A, et al. Evidence-based management of chylothorax in infants[J]. J Pediatr Surg, 2017, 52(6): 907-912.
doi: S0022-3468(17)30159-8 pmid: 28342580 |
| [29] |
Drolet BA, Frommelt PC, Chamlin SL, et al. Initiation and use of propranolol for infantile hemangioma: report of a consensus conference[J]. Pediatrics, 2013, 131(1): 128-140.
doi: 10.1542/peds.2012-1691 pmid: 23266923 |
| [30] |
Ozeki M, Kanda K, Kawamoto N, et al. Propranolol as an alternative treatment option for pediatric lymphatic malformation[J]. Tohoku J Exp Med, 2013, 229(1): 61-66.
pmid: 23257321 |
| [31] |
Thornbury KD, McHale NG, McGeown JG. Alpha-and beta-components of the popliteal efferent lymph flow response to intra-arterial catecholamine infusions in the sheep[J]. Blood Vessels, 1989, 26(2): 107-118.
pmid: 2758107 |
| [32] | Omri S, Tahiri H, Pierre WC, et al. Propranolol attenuates proangiogenic activity of mononuclear phagocytes: implication in choroidal neovascularization[J]. Invest Ophthalmol Vis Sci, 2019, 60(14): 4632-4642. |
| [33] | Handal-Orefice R, Midura D, Wu JK, et al. Propranolol therapy for congenital chylothorax[J]. Pediatrics, 2023, 151(2): e2022058555. |
| [34] | Corda R, Chrisomalis-Dring S, Crook S, et al. Propranolol treatment for chylothorax after congenital cardiac surgery[J]. J Thorac Cardiovasc Surg, 2022, 163(5): 1630-1641. |
| [1] | ZHENG Nuo, CHEN Man, ZHANG Dongli, LIU Xiaoming. Diagnosis and treatment of one case of refractory neuromyelitis optica spectrum disorder in adolescents [J]. Journal of Clinical Pediatrics, 2025, 43(4): 301-305. |
| [2] | HUANG Jing, LIU Xiaochen, GAO Xiong, LI Xiaowen, LI Guanghong, LI Luquan. The value of measuring trace elements and oxidative/antioxidant factors in umbilical blood in predicting the onset and evaluation of neonatal respiratory distress syndrome [J]. Journal of Clinical Pediatrics, 2025, 43(3): 204-210. |
| [3] | WU Jianqiang, SHEN Danping, LU Meiping. Salvage therapy for refractory macrophage activation syndrome associated with systemic juvenile idiopathic arthritis: a case report [J]. Journal of Clinical Pediatrics, 2025, 43(3): 216-219. |
| [4] | HE Ying, LIU Zhiyong, YANG Hansong, CAI Yali, XU Jinglin, CHEN Dongmei. Clinical analysis of 153 neonatal enterovirus infections and antibiotic management improvement study [J]. Journal of Clinical Pediatrics, 2025, 43(2): 128-134. |
| [5] | NI Yongan, SUN Lirong. Research advances in the treatment of refractory Langerhans cell histiocytosis [J]. Journal of Clinical Pediatrics, 2025, 43(10): 798-802. |
| [6] | LIU Dongxia, JIN Rong, LIN Rongjun. Risk factors analysis of severe refractory Mycoplasma pneumoniae pneumonia complicated with bronchitis obliterans in children [J]. Journal of Clinical Pediatrics, 2025, 43(1): 29-34. |
| [7] | ZHANG Ruijie, XI Guannan, WANG Xuefeng, LIN Xin’ao, DAI Jiale, FAN Xiaobo, WANG Jimei. Application of simplified lung ultrasound performed shortly after birth in the respiratory support needs of late preterm and term infants [J]. Journal of Clinical Pediatrics, 2024, 42(8): 714-721. |
| [8] | WANG Yu, XUE Yujuan, ZUO Yingxi, JIA Yueping, LU Aidong, ZENG Huimin, ZHANG Leping. Efficacy and safety of CD19 targeted CAR-T cells in the treatment of refractory/relapsed B-cell acute lymphoblastic leukemia in children and adolescents [J]. Journal of Clinical Pediatrics, 2024, 42(7): 583-588. |
| [9] | SHANG Qianwen, ZHANG Yongzhan, LU Aidong, JIA Yueping, ZUO Yingxi, DING Mingming, ZHANG Leping, ZENG Huimin. The efficacy and safety of modified CLAG regimen for relapsed or refractory acute myeloid leukemia in children [J]. Journal of Clinical Pediatrics, 2024, 42(7): 589-594. |
| [10] | WANG Man, LI Luquan, LI Xiaowen. Analysis of risk factors for early-onset sepsis associated acute kidney injury in neonates [J]. Journal of Clinical Pediatrics, 2024, 42(6): 520-525. |
| [11] | ZHOU Yiping, DOU Jiaying, CUI Yun, SHI Jingyi, SUN Ting, ZHANG Yucai. Clinical analysis of the first refractory status epilepticus in pediatric intensive care unit [J]. Journal of Clinical Pediatrics, 2024, 42(5): 439-444. |
| [12] | YANG Lei, FANG Fang, SONG Tianyu, XU Chaolong. A clinical and prognosis study of five patients with cerebral creatine deficiency syndrome 2 caused by GAMT gene mutations [J]. Journal of Clinical Pediatrics, 2024, 42(12): 1039-1046. |
| [13] | YANG Liu, SU Meng, ZHANG Jing, AN Kang, CAI Jiaoyang, QIAN Juan, TANG Yanjing, LI Benshang. Clinical analysis of CD19/CD22 CAR-T cell therapy for MLL gene rearrangement-positive refractory/relapsed childhood acute B-lineage lymphoblastic leukemia [J]. Journal of Clinical Pediatrics, 2024, 42(10): 888-894. |
| [14] | XIANG Chao, ZHANG Rong, KANG Lan, LEI Xiaoping, LIU Xingqing, DONG Wenbin. Association of coefficient of glycemic variation and SNAPPE-Ⅱ with prognosis in critically ill neonates [J]. Journal of Clinical Pediatrics, 2023, 41(6): 430-435. |
| [15] | XU Jinglin, YANG Hansong, CHEN Xinhua, CHEN Jiangbin, LI Xiaoqing, ZHANG Weifeng, CHEN Dongmei. Clinical analysis of continuous blood purification in the treatment of neonatal septic shock with acute kidney injury [J]. Journal of Clinical Pediatrics, 2023, 41(6): 436-441. |
|
||