

Journal of Clinical Pediatrics ›› 2023, Vol. 41 ›› Issue (3): 204-209.doi: 10.12372/jcp.2023.22e0067
• Hematology and Oncology Disease • Previous Articles Next Articles
XUE Yujuan, LU Aidong, WANG Yu, JIA Yueping, ZUO Yingxi, ZHANG Leping( )
)
Received:2022-01-11
Published:2023-03-15
Online:2023-03-10
XUE Yujuan, LU Aidong, WANG Yu, JIA Yueping, ZUO Yingxi, ZHANG Leping. Clinical analysis of treatment failure in children with acute lymphoblastic leukemia[J].Journal of Clinical Pediatrics, 2023, 41(3): 204-209.
"
| 临床特征 | 例数 | 复发时间 | 复发部位 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 极早期 | 早期 | 晚期 | χ2值 | P | 骨髓 | 中枢神经系统 | 骨髓+中枢神经系统 | 其他髓外复发 | χ2值 | P | ||
| 性别 | 2.25 | 0.324 | - | 0.6191) | ||||||||
| 男 | 73 | 33(45.2) | 27(37.0) | 13(17.8) | 58(79.5) | 5(6.8) | 8(11.0) | 2(2.7) | ||||
| 女 | 31 | 19(61.3) | 8(25.8) | 4(12.9) | 26(83.9) | 3(9.7) | 1(3.2) | 1(3.2) | ||||
| 年龄/岁 | 0.43 | 0.808 | - | 0.7911) | ||||||||
| ≥10 | 44 | 23(52.3) | 15(34.1) | 6(13.6) | 34(77.3) | 4(9.1) | 5(11.4) | 1(2.3) | ||||
| 1~10 | 60 | 29(48.3) | 20(33.3) | 11(18.3) | 50(83.3) | 4(6.7) | 4(6.7) | 2(3.3) | ||||
| 初诊WBC×109·L-1 | 7.53 | 0.023 | - | 0.0111) | ||||||||
| ≥50.0 | 33 | 23(69.7) | 7(21.2) | 3(9.1) | 23(69.7) | 3(9.1) | 7(21.2) | 0(0.0) | ||||
| <50.0 | 71 | 29(40.8) | 28(39.4) | 14(19.7) | 61(85.9) | 5(7.0) | 2(2.8) | 3(4.2) | ||||
| 免疫分型 | - | 0.0191) | - | 0.0161) | ||||||||
| B-ALL | 88 | 39(44.3) | 32(36.4) | 17(19.3) | 74(84.1) | 7(8.0) | 4(4.5) | 3(3.4) | ||||
| T-ALL | 16 | 13(81.3) | 3(18.8) | 0(0.0) | 10(62.5) | 1(6.3) | 5(31.3) | 0(0.0) | ||||
| 融合基因 | - | 0.0221) | - | 0.5451) | ||||||||
| ETV6-RUNX1+ | 6 | 0(0.0) | 4(66.7) | 2(33.3) | 5(83.3) | 0(0.0) | 0(0.0) | 1(16.7) | ||||
| MLL+ | 2 | 1(50.0) | 0(0.0) | 1(50.0) | 2(100.0) | 0(0.0) | 0(0.0) | 0(0.0) | ||||
| E2A-PBX1+ | 8 | 4(50.0) | 1(12.5) | 3(37.5) | 6(75.0) | 2(25.0) | 0(0.0) | 0(0.0) | ||||
| BCR-ABL1+ | 9 | 7(77.8) | 2(22.2) | 0(0.0) | 7(77.8) | 1(11.1) | 1(11.1) | 0(0.0) | ||||
| 其他 | 79 | 40(50.6) | 28(35.4) | 11(13.9) | 64(81.0) | 5(6.3) | 8(10.1) | 2(2.5) | ||||
| 第15天骨髓原始 幼稚淋巴细胞/% | 1.71 | 0.426 | - | 0.8191) | ||||||||
| <5.0 | 44 | 21(47.7) | 13(29.5) | 10(22.7) | 34(77.3) | 4(9.1) | 5(11.4) | 1(2.3) | ||||
| ≥5.0 | 46 | 27(58.7) | 13(28.3) | 6(13.0) | 39(84.8) | 3(6.5) | 3(6.5) | 1(2.2) | ||||
| 未检测 | 14 | 4(28.6) | 9(64.3) | 1(7.1) | 11(78.6) | 1(7.1) | 1(7.1) | 1(7.1) | ||||
| 第33天MRD/% | 3.35 | 0.780 | - | 0.8791) | ||||||||
| ≥1.0 | 21 | 11(52.4) | 7(33.3) | 3(14.3) | 17(81.0) | 1(4.8) | 2(9.5) | 1(4.8) | ||||
| 0.1~1.0 | 24 | 14(58.3) | 5(20.8) | 5(20.8) | 22(91.7) | 1(4.2) | 1(4.2) | 0(0.0) | ||||
| 0.01~0.1 | 10 | 4(40.0) | 5(50.0) | 1(10.0) | 9(90.0) | 0(0) | 1(10.0) | 0(0.0) | ||||
| <0.01 | 49 | 23(46.9) | 18(36.7) | 8(16.3) | 36(73.5) | 6(12.2) | 5(10.2) | 2(4.1) | ||||
| 第90天MRD/% | - | 0.1291) | - | 0.3361) | ||||||||
| ≥0.1 | 17 | 13(76.5) | 3(17.6) | 1(5.9) | 16(94.1) | 0(0.0) | 0(0.0) | 1(5.9) | ||||
| 0.01~0.1 | 10 | 6(60.0) | 2(20.0) | 2(20.0) | 10(100.0) | 0(0.0) | 0(0.0) | 0(0.0) | ||||
| <0.01 | 77 | 33(42.9) | 30(39.0) | 14(18.2) | 58(75.3) | 8(10.4) | 9(11.7) | 2(2.6) | ||||
| 复发部位 | - | 0.3211) | - | - | ||||||||
| 骨髓 | 84 | 45(53.6) | 25(29.8) | 14(16.7) | - | - | - | |||||
| 中枢神经系统 | 8 | 3(37.5) | 3(37.5) | 2(25) | - | - | - | |||||
| 骨髓+中枢神经系统 | 9 | 4(44.4) | 4(44.4) | 1(11.1) | - | - | - | |||||
| 其他髓外复发 | 3 | 0(0.0) | 3(100.0) | 0(0.0) | ||||||||
| 危险度 | - | 0.0291) | - | 0.0531) | ||||||||
| 标危 | 11 | 2(18.2) | 7(63.6) | 2(18.2) | 8(72.7) | 0(0.0) | 1(9.1) | 2(18.2) | ||||
| 中危 | 52 | 23(44.2) | 18(34.6) | 11(21.2) | 41(78.8) | 7(13.5) | 4(7.7) | 0(0.0) | ||||
| 高危 | 41 | 27(65.9) | 10(24.4) | 4(9.8) | 35(85.4) | 1(2.4) | 4(9.8) | 1(2.4) | ||||
"
| 预后因素 | 失败例数 | 3年OS率/% | χ2值 | P | 3年TFS率/% | χ2值 | P |
|---|---|---|---|---|---|---|---|
| 性别 | 0.25 | 0.621 | 1.91 | 0.167 | |||
| 男 | 82 | 87.2±1.7 | 81.7±2.0 | ||||
| 女 | 42 | 87.0±2.1 | 84.9±2.3 | ||||
| 年龄/岁 | 15.00 | 0.001 | 11.82 | 0.003 | |||
| ≥10 | 54 | 79.3±2.9 | 75.3±3.1 | ||||
| 1~10 | 70 | 90.6±1.4 | 86.3±1.6 | ||||
| 初诊WBC×109·L-1 | 10.41 | 0.001 | 10.60 | 0.001 | |||
| ≥50.0 | 39 | 77.9±3.6 | 73.6±3.8 | ||||
| <50.0 | 85 | 89.7±1.4 | 85.5±1.6 | ||||
| 免疫分型 | 12.98 | <0.001 | 7.04 | 0.008 | |||
| T-ALL | 23 | 72.8±5.1 | 70.3±5.2 | ||||
| B-ALL | 101 | 89.1±1.3 | 84.7±1.5 | ||||
| 融合基因 | 38.42 | <0.001 | 38.85 | <0.001 | |||
| ETV6/RUNX1+ | 6 | 97.8±1.6 | 95.7±2.1 | ||||
| MLL+ | 3 | 91.7±5.6 | 91.7±5.6 | ||||
| E2A/PBX1+ | 11 | 89.7±4.9 | 79.5±6.5 | ||||
| BCR/ABL1+ | 13 | 77.7±5.9 | 74.0±6.2 | ||||
| 其他 | 91 | 85.6±1.8 | 81.1±2.0 | ||||
| 伴髓外浸润 | 7.42 | 0.006 | 3.69 | 0.055 | |||
| 是 | 13 | 74.4±6.7 | 74.4±6.7 | ||||
| 否 | 111 | 88.0±1.4 | 83.6±1.5 | ||||
| 第15天骨髓原始幼稚淋巴细胞/%1) | 23.63 | <0.001 | 32.23 | <0.001 | |||
| ≥5.0 | 55 | 78.2±3.2 | 70.5±3.5 | ||||
| <5.0 | 52 | 92.0±1.4 | 89.4±1.6 | ||||
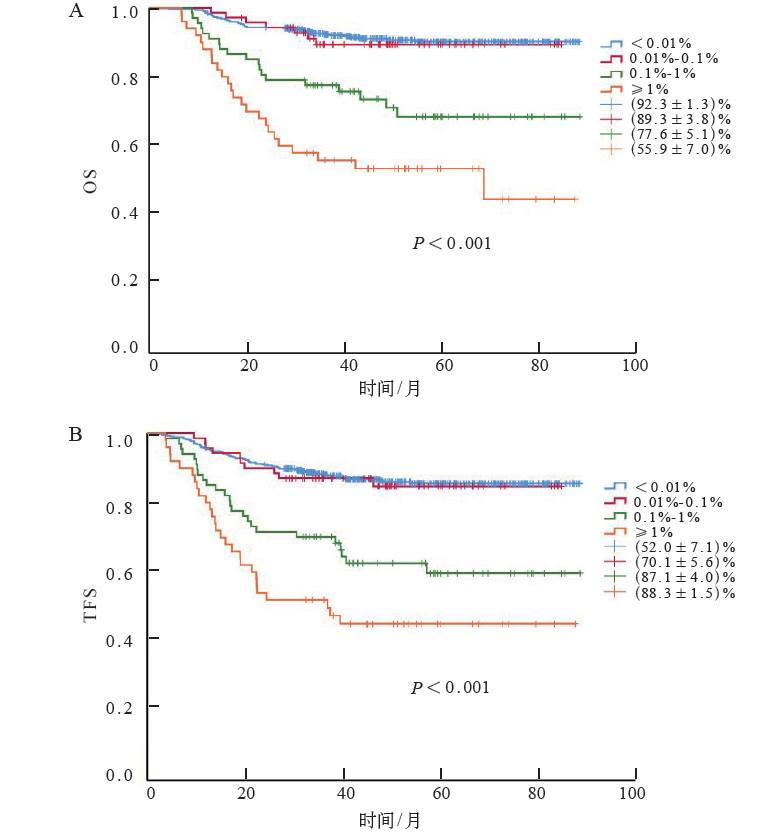
| 第33天MRD/%2) | 80.00 | <0.001 | 76.43 | <0.001 | |||
| ≥1.0 | 27 | 55.9±7.0 | 52.0±7.1 | ||||
| 0.1~1.0 | 25 | 77.6±5.1 | 70.1±5.6 | ||||
| 0.01~0.1 | 10 | 89.3±3.8 | 87.1±4.0 | ||||
| <0.01 | 59 | 92.3±1.3 | 88.3±1.5 | ||||
| 90天MRD/%3) | 47.29 | <0.001 | 55.68 | <0.001 | |||
| ≥0.1 | 18 | 53.1±8.8 | 46.9±8.8 | ||||
| 0.01~0.1 | 10 | 76.0±8.5 | 68.0±9.3 | ||||
| <0.01 | 92 | 90.1±1.3 | 86.2±1.5 | ||||
| 危险度分层 | 53.46 | <0.001 | 47.01 | <0.001 | |||
| 标危 | 13 | 97.0±1.3 | 93.6±1.9 | ||||
| 中危 | 60 | 88.7±1.8 | 84.0±2.1 | ||||
| 高危 | 51 | 70.8±3.8 | 66.7±4.0 |

"
| [1] |
Zheng R, Peng X, Zeng H, et al. Incidence, mortality and survival of childhood cancer in China during 2000-2010 period: a population-based study[J]. Cancer Lett, 2015, 363(2): 176-180.
doi: 10.1016/j.canlet.2015.04.021 pmid: 25917566 |
| [2] |
Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014[J]. CA Cancer J Clin, 2014, 64(2): 83-103.
doi: 10.3322/caac.21219 |
| [3] |
Inaba H, Mullighan CG. Pediatric acute lymphoblastic leukemia[J]. Haematologica, 2020, 105(11): 2524-2539.
doi: 10.3324/haematol.2020.247031 pmid: 33054110 |
| [4] |
Kato M, Manabe A. Treatment and biology of pediatric acute lymphoblastic leukemia[J]. Pediatr Int, 2018, 60(1): 4-12.
doi: 10.1111/ped.13457 pmid: 29143423 |
| [5] | 张之南, 沈悌. 血液病诊断及疗效标准[M]. 北京: 科学出版社, 2007. |
| [6] | 李宗儒, 赵婷, 刘艳荣, 等. 微小残留病在高危Ph阴性急性淋巴细胞白血病中的意义[J]. 中华血液学杂志, 2019, 40(7): 554-560. |
| [7] |
Xue YJ, Wang Y, Jia YP, et al. The role of minimal residual disease in specific subtypes of pediatric acute lymphoblastic leukemia[J]. Int J Hematol, 2021, 113(4): 547-555.
doi: 10.1007/s12185-020-03063-w |
| [8] |
Inaba H, Pui CH. Advances in the diagnosis and treatment of pediatric acute lymphoblastic leukemia[J]. J Clin Med, 2021, 10(9): 1926.
doi: 10.3390/jcm10091926 |
| [9] |
Cui L, Li ZG, Chai YH, et al. Outcome of children with newly diagnosed acute lymphoblastic leukemia treated with CCLG-ALL 2008: the first nation-wide prospective multicenter study in China[J]. Am J Hematol, 2018, 93(7): 913-920.
doi: 10.1002/ajh.25124 pmid: 29675840 |
| [10] | 朱嘉莳, 李红, 邵静波, 等. 急性淋巴细胞白血病儿童治疗失败原因的分析[J]. 上海交通大学学报(医学版), 2021, 41(6): 764-769. |
| [11] |
Jaime-Pérez JC, Pinzón-Uresti MA, Jiménez-Castillo RA, et al. Relapse of childhood acute lymphoblastic leukemia and outcomes at a reference center in Latin America: organomegaly at diagnosis is a significant clinical predictor[J]. Hematology, 2018, 23(1): 1-9.
doi: 10.1080/10245332.2017.1333294 pmid: 28580844 |
| [12] |
Oskarsson T, Söderhäll S, Arvidson J, et al. Relapsed childhood acute lymphoblastic leukemia in the Nordic countries: prognostic factors, treatment and outcome[J]. Haematologica, 2016, 101(1): 68-76.
doi: 10.3324/haematol.2015.131680 pmid: 26494838 |
| [13] | 高伟, 蒋梦影, 高莉, 等. 儿童急性淋巴细胞白血病治疗失败的相关因素分析[J]. 中国实验血液学杂志, 2021, 29(3): 661-668. |
| [14] |
Gaudichon J, Jakobczyk H, Debaize L, et al. Mechanisms of extramedullary relapse in acute lymphoblastic leukemia: reconciling biological concepts and clinical issues[J]. Blood Rev, 2019, 36: 40-56.
doi: S0268-960X(18)30078-X pmid: 31010660 |
| [15] |
Lenk L, Alsadeq A, Schewe DM. Involvement of the central nervous system in acute lymphoblastic leukemia: opinions on molecular mechanisms and clinical implications based on recent data[J]. Cancer Metastasis Rev, 2020, 39(1): 173-187.
doi: 10.1007/s10555-020-09848-z |
| [16] | Yu X, Zhang H, Yuan M, et al. Identification and characterization of a murine model of BCR-ABL1+ acute B-lymphoblastic leukemia with central nervous system metastasis[J]. Oncol Rep, 2019, 42(2): 521-532. |
| [17] |
Liao C, Xu X, Shen D, et al. Minimal residual disease-guided risk restratification and therapy improves the survival of childhood acute lymphoblastic leukemia: experience from a tertiary children's hospital in China[J]. J Pediatr Hematol Oncol, 2019, 41(6): e346-e354.
doi: 10.1097/MPH.0000000000001412 |
| [18] |
Campana D, Pui CH. Minimal residual disease-guided therapy in childhood acute lymphoblastic leukemia[J]. Blood, 2017, 129(14): 1913-1918.
doi: 10.1182/blood-2016-12-725804 pmid: 28167658 |
| [19] | 冯静, 陈晓娟, 刘晓明, 等. 多参数流式细胞术检测的微小残留病与儿童急性B淋巴细胞白血病预后的相关性研究[J]. 中华血液学杂志, 2019, 40(8): 678-680. |
| [20] |
Borowitz MJ, Wood BL, Devidas M, et al. Prognostic significance of minimal residual disease in high risk B-ALL: a report from Children's Oncology Group study AALL0232[J]. Blood, 2015, 126(8): 964-971.
doi: 10.1182/blood-2015-03-633685 pmid: 26124497 |
| [21] |
Pui CH, Pei D, Coustan-Smith E, et al. Clinical utility of sequential minimal residual disease measurements in the context of risk-based therapy in childhood acute lymphoblastic leukaemia: a prospective study[J]. Lancet Oncol, 2015, 16(4): 465-474.
doi: 10.1016/S1470-2045(15)70082-3 |
| [22] |
Inaba H, Pui CH. Immunotherapy in pediatric acute lymphoblastic leukemia[J]. Cancer Metastasis Rev, 2019, 38(4): 595-610.
doi: 10.1007/s10555-019-09834-0 |
| [23] |
O'Connor D, Bate J, Wade R, et al. Infection-related mortality in children with acute lymphoblastic leukemia: an analysis of infectious deaths on UKALL2003[J]. Blood, 2014, 124(7): 1056-1061.
doi: 10.1182/blood-2014-03-560847 pmid: 24904116 |
| [24] |
Inaba H, Pei D, Wolf J, et al. Infection-related com-plications during treatment for childhood acute lymphoblastic leukemi a[J]. Ann Oncol, 2017, 28(2): 386-392.
doi: 10.1093/annonc/mdw557 pmid: 28426102 |
| [1] | ZHAO Min, TANG Jihong, XIAO Xiao, YANG Letian, XU Huan, WU Yinyin, FENG Juan. Acute lymphoblastic leukemia with chemotherapy-related cerebral lesion: clinical and imaging features [J]. Journal of Clinical Pediatrics, 2025, 43(1): 14-20. |
| [2] | LUO Mingjing, YU Jiaming, WANG Xiaodong, ZHANG Xiaoling, YU Yue, ZHANG Yu, WEN Feiqiu, LIU Sixi. Clinical analysis of invasive fungal disease secondary to allogeneic hematopoietic stem cell transplantation in 424 children with thalassemia [J]. Journal of Clinical Pediatrics, 2025, 43(1): 21-28. |
| [3] | LIU Dongxia, JIN Rong, LIN Rongjun. Risk factors analysis of severe refractory Mycoplasma pneumoniae pneumonia complicated with bronchitis obliterans in children [J]. Journal of Clinical Pediatrics, 2025, 43(1): 29-34. |
| [4] | ZHONG Jinhong, WANG Can, CHEN Fang. Progress in the research of infantile fiberoptic bronchoscopy sedation [J]. Journal of Clinical Pediatrics, 2025, 43(1): 50-55. |
| [5] | JIANG Weiqin, WANG Jing, CHENG Anna, CHEN Tingting, HUANG Yujuan. Predictors of recurrent febrile seizures during the same febrile illness in children with febrile seizures [J]. Journal of Clinical Pediatrics, 2025, 43(1): 8-13. |
| [6] | QIU Xiu, WEI Dongmei, LIN Shanshan, XIA Huimin, ZHOU Wenhao. Principles and practice of the Born in Guangzhou Cohort Study [J]. Journal of Clinical Pediatrics, 2024, 42(9): 747-752. |
| [7] | FAN Jianxia. The origins and development of the healthy life trajectory program: a cohort of community-family-mother-child multidimensional interventions for overweight and obesity in children [J]. Journal of Clinical Pediatrics, 2024, 42(9): 768-773. |
| [8] | JIANG Tao, LI Shuangjie, TANG Lian, OUYANG Wenxian. Immunobiological properties of peripheral blood MAIT cells in children with chronic hepatitis B [J]. Journal of Clinical Pediatrics, 2024, 42(9): 787-790. |
| [9] | ZHOU Jie, LIU Keqiang, WANG Jinling, WANG Ying. Megacystis-microcolon-intestinal hypoperistalsis syndrome caused by MYH11 elongating mutation : a case report and literatures review [J]. Journal of Clinical Pediatrics, 2024, 42(9): 798-804. |
| [10] | CHU Sijia, TANG Jihong. Research progress of central nervous system injury associated with pediatric acute lymphoblastic leukemia and its treatment [J]. Journal of Clinical Pediatrics, 2024, 42(9): 811-816. |
| [11] | DING Yaping, XIA Shanshan, ZHANG Chenmei. Interpretation of “2023 Children’s Renal Nutrition Working Group Clinical Practice Recommendations: Nutritional Management of Children with Acute Kidney Injury” [J]. Journal of Clinical Pediatrics, 2024, 42(8): 667-672. |
| [12] | LI Yirong, LI Huiping, GAO Jingyu, XIAO Yuhua, CHEN Xiaomin, LU Yanling, ZHAO Nana, FENG Xiaoqin. Comparison of different doses of cytarabine for induction chemotherapy in children with acute myeloid leukemia in FLAG-IDA regimen [J]. Journal of Clinical Pediatrics, 2024, 42(8): 673-677. |
| [13] | HUANG Bo, DONG Yanying, SONG Linlan. Clinical characteristics of 348 children with infectious mononucleosis [J]. Journal of Clinical Pediatrics, 2024, 42(8): 678-683. |
| [14] | WANG Dan, SHAO Jingbo, LI Hong, ZHANG Na, ZHU Jiashi, FU Pan, WANG Zhen. Clinical analysis of 38 cases of hematological malignancies complicated with tumor lysis syndrome in children [J]. Journal of Clinical Pediatrics, 2024, 42(8): 684-690. |
| [15] | MA Yan, WEI Xingjiao, BAI Hua, ZHANG Yan, TIAN Xinmin, Aqsa Ahmad, LIANG Lijun. Analysis of etiological composition and clinical features of stage 5 chronic kidney disease in children in a tertiary hospital in western China [J]. Journal of Clinical Pediatrics, 2024, 42(8): 697-703. |
|
||