

Journal of Clinical Pediatrics ›› 2026, Vol. 44 ›› Issue (6): 489-498.doi: 10.12372/jcp.2026.26e0076
• Original Article • Previous Articles Next Articles
LIU Ziyao1,2, WANG Congying2, WANG Hongmao2, ZHANG Mingming2, XU Yingjie3, LAI Jianming3, NIU Wenquan4, LI Xiaohui1,5( )
)
Received:2026-01-23
Revised:2026-04-01
Accepted:2026-04-16
Published:2026-06-15
Online:2026-06-04
Contact:
LI Xiaohui
E-mail:lxhmaggie@pumc.edu.cn
CLC Number:
LIU Ziyao, WANG Congying, WANG Hongmao, ZHANG Mingming, XU Yingjie, LAI Jianming, NIU Wenquan, LI Xiaohui. Early differentiation of Kawasaki disease with joint symptoms and systemic juvenile idiopathic arthritis with Kawasaki disease-like symptoms: a single-center retrospective study[J].Journal of Clinical Pediatrics, 2026, 44(6): 489-498.

Figure 1
Flowchart of patient enrollment"
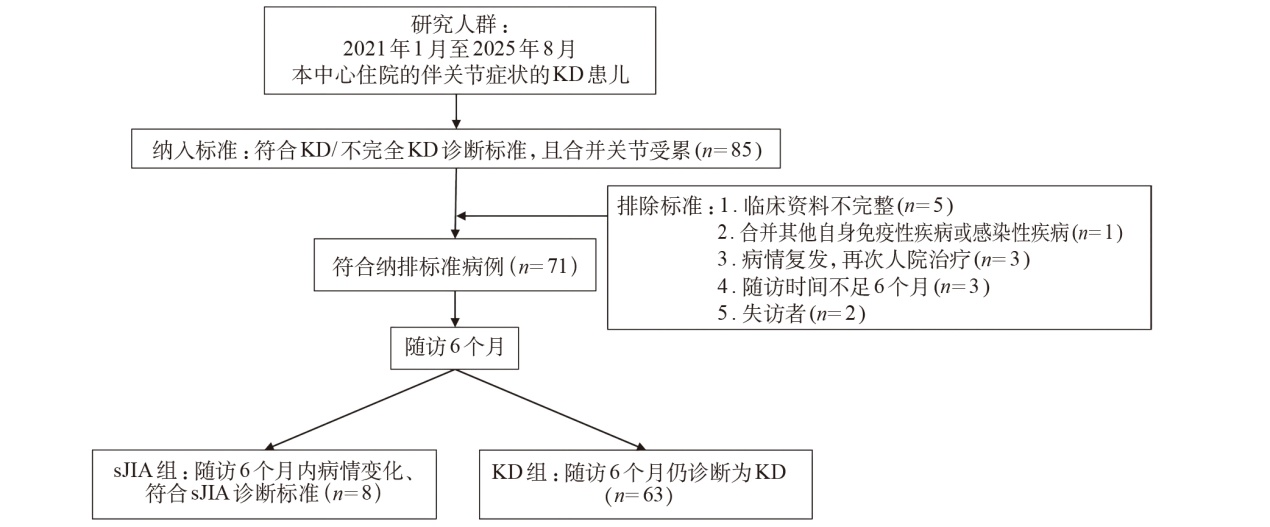
Table 1
Comparison of clinical characteristics between KD group and sJIA group"
| 项 目 | KD组(n=63) | sJIA组(n=8) | 统计量 | P |
|---|---|---|---|---|
| 初诊时 | ||||
| 起病年龄[M(P25~P75)]/岁 | 4.3(2.4~5.2) | 4.0(3.3~4.5) | Z=0.32 | 0.750 |
| 男性[n(%)] | 41(65.1) | 5(62.5) | χ2=0.00 | 1.000 |
| 发热持续时间[M(P25~P75)]/d | 8.0(7.0~11.0) | 24.5(20.5~30.0) | Z=3.58 | <0.001 |
| 起病至关节症状出现/发现时间[M(P25~P75)]/d | 9.0(6.5~12.0) | 12.5(6.5~18.5) | Z=1.11 | 0.266 |
| Kobayashi评分[M(P25~P75)] | 2.0(0.0~5.0) | 5.0(3.5~6.0) | Z=1.57 | 0.116 |
| CRP[M(P25~P75)]/mg·L-1 | 87.0 (46.2~127.4) | 70.7(57.0~107.4) | Z=0.45 | 0.656 |
| IVIg治疗后CRP[M(P25~P75)]/mg·L-1 | 12.9(4.5~30.1) | 61.0(45.2~72.7) | Z=3.48 | <0.001 |
| ΔCRP[M(P25~P75)]/mg·L-1 | 66.4(28.3~99.9) | 15.2(9.0~34.2) | Z=2.89 | 0.011 |
| CRP下降率[M(P25~P75)]/% | 0.8(0.7~0.9) | 0.2(0.1~0.5) | Z=3.88 | <0.001 |
| ESR[M(P25~P75)]/mm·h-1 | 72.5(48.0~83.3) | 74.5(69.3~75.5) | Z=0.27 | 0.789 |
| 铁蛋白[M(P25~P75)]/ng·mL-1 | 300.7(214.3~376.1) | 394.2(253.8~1152.2) | Z=1.16 | 0.246 |
| 纤维蛋白原[M(P25~P75)]/g·L-1 | 5.4(4.5~6.8) | 4.6(3.8~6.3) | Z=1.09 | 0.275 |
| 白细胞计数[M(P25~P75)]/×109·L-1 | 12.8(10.8~17.0) | 9.9(7.7~13.2) | Z=1.61 | 0.108 |
| 血红蛋白( x±s)/g·L-1 | 110.8±9.1 | 106.4±18.0 | t=0.69 | 0.511 |
| 血小板计数[M(P25~P75)]/×109·L-1 | 367.0(291.0~463.5) | 328.0(297.8~505.0) | Z=0.06 | 0.949 |
| AST[M(P25~P75)]/U·L-1 | 23.5(18.6~31.3) | 32.5(28.1~59.2) | Z=2.25 | 0.025 |
| ALT[M(P25~P75)]/U·L-1 | 21.4(13.8~66.2) | 22.3(17.2~112.6) | Z=0.49 | 0.623 |
| LDH[M(P25~P75)]/U·L-1 | 224.0(194.5~258.5) | 230.5(214.5~282.5) | Z=0.76 | 0.445 |
| IL-6[M(P25~P75)]/pg·mL-1 | 33.7(14.1~173.0) | 69.1(38.2~156.4) | Z=0.65 | 0.518 |
| IL-1β[M(P25~P75)]/pg·mL-1 | 9.0(5.0~16.5) | 8.8(3.7~15.4) | Z=0.56 | 0.575 |
| TNF-α[M(P25~P75)]/pg·mL-1 | 23.1(14.6~32.8) | 18.4(4.9~33.1) | Z=1.03 | 0.304 |
| 受累关节数[M(P25~P75)]/个 | 2.0(1.0~4.0) | 5.5(3.75~20.0) | Z=2.91 | 0.004 |
| 冠状动脉瘤[n(%)] | 8(12.7) | 1(12.5) | χ2=0.00 | 1.000 |
| MAS[n(%)] | 0(0.0) | 0(0.0) | - | - |
| 随访1个月 | ||||
| CRP[M(P25~P75)]/mg·L-1 | 4.9(1.3~8.9) | 33.2(26.7~43.4) | Z=4.21 | <0.001 |
| 受累关节数[M(P25~P75)]/个 | 0.0(0.0~1.0) | 4.0(3.0~13.0) | Z=4.50 | <0.001 |
| 冠状动脉瘤[n(%)] | 6(9.5) | 0(0.0) | - | 1.0001) |
| MAS[n(%)] | 0(0.0) | 1(12.5) | - | 0.1131) |
| 随访6个月 | ||||
| CRP[M(P25~P75)]/mg·L-1 | 1.7(0.6~3.7) | 0.9(0.7~2.7) | Z=0.77 | 0.440 |
| 受累关节数[M(P25~P75)]/个 | 0.0(0.0~0.0) | 3.0(1.0~8.0) | Z=5.14 | <0.001 |
| 冠状动脉瘤[n(%)] | 1(1.7) | 0(0.0) | - | 1.0001) |
| MAS[n(%)] | 0(0.0) | 0(0.0) | - | - |
Figure 2
The ROC curve for differentiating the sJIA group from the KD group by the duration of fever, the involved joints numbers"
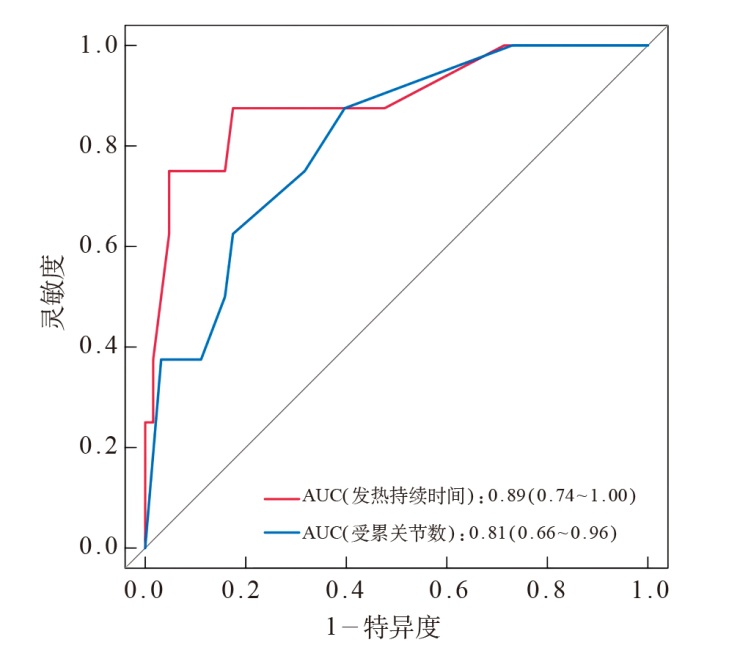
Table 2
Comparison of joint involvement in children between the sJIA and KD groups [n(%)]"
| 项 目 | KD组(n=63) | sJIA组(n=8) | χ2值 | P |
|---|---|---|---|---|
| 按关节症状出现/发现时间分类 | 0.11 | 0.739 | ||
| 早发型关节炎 | 32(50.8) | 3(37.5) | ||
| 晚发型关节炎 | 31(49.2) | 5(62.5) | ||
| 按关节数量分类 | 5.87 | 0.015 | ||
| 少关节炎 | 52(82.5) | 3(37.5) | ||
| 多关节炎 | 11(17.5) | 5(62.5) | ||
| 按关节种类分类 | - | <0.0011) | ||
| 大关节炎 | 55(87.3) | 1(12.5) | ||
| 小关节炎 | 2(3.2) | 0(0.0) | ||
| 混合型关节炎 | 6(9.5) | 7(87.5) | ||
| 具体受累关节 | ||||
| 髋 | 37(58.7) | 7(87.5) | 1.42 | 0.233 |
| 膝 | 34(53.97) | 7(87.5) | 2.04 | 0.153 |
| 踝 | 20(31.8) | 3(37.5) | 0.00 | 1.000 |
| 腕 | 8(12.7) | 4(50.0) | 4.63 | 0.031 |
| 肘 | 3(4.76) | 0(0.0) | - | 1.0001) |
| 肩 | 3(4.76) | 1(12.5) | - | 0.3871) |
| 指 | 5(7.9) | 4(50.0) | 7.86 | 0.005 |
| 趾 | 2(3.2) | 1(12.5) | - | 0.3051) |
| 影像学表现 | ||||
| 关节积液 | 52(82.5) | 6(75.0) | 0.00 | 0.973 |
| 滑膜增厚 | 16(25.4) | 6(75.0) | 6.01 | 0.014 |
| 软组织水肿 | 12(19.1) | 3(37.5) | 0.55 | 0.456 |
| 骨髓水肿 | 0(0.0) | 1(12.5) | - | 0.1131) |
| 骨质破坏 | 0(0.0) | 0(0.0) | - | - |
Table 3
Analysis of treatment response and medications between the sJIA and KD groups [n(%)]"
| 项 目 | KD组(n=63) | sJIA组(n=8) | χ2值 | P |
|---|---|---|---|---|
| IVIg | 63(100.0) | 8(100.0) | - | - |
| IVIg无反应 | 24(38.1) | 8(100.0) | 8.63 | 0.003 |
| DMARDs | 0(0.0) | 8(100.0) | - | <0.0011) |
| 糖皮质激素 | 25(39.7) | 8(100.0) | 8.10 | 0.004 |
| 生物制剂 | 5(7.9) | 6(75.0) | 19.53 | <0.001 |
| 英夫利昔单抗 | 5(7.9) | 2(25.0) | - | 0.1751) |
| 托珠单抗 | 0(0.0) | 3(37.5) | - | <0.0011) |
| 托法替布 | 0(0.0) | 1(12.5) | - | 0.1131) |
| 治疗组合 | ||||
| IVIg单用 | 35(55.6) | 0(0.0) | 6.68 | 0.010 |
| IVIg+糖皮质激素 | 23(36.5) | 0(0.0) | 2.81 | 0.093 |
| IVIg+生物制剂 | 3(4.8) | 0(0.0) | - | 1.0001) |
| IVIg+糖皮质激素+生物制剂 | 2(3.2) | 0(0.0) | - | 1.0001) |
| IVIg+糖皮质激素+DMARDs | 0(0.0) | 2(25.0) | - | 0.0111) |
| IVIg+生物制剂+DMARDs | 0(0.0) | 0(0.0) | - | - |
| IVIg+糖皮质激素+生物制剂+DMARDs | 0(0.0) | 6(75.0) | - | <0.0011) |
Table 4
Analysis of coronary artery involvement between the sJIA and KD groups"
| 项 目 | KD组(n=63) | sJIA组(n=8) | 统计量 | P |
|---|---|---|---|---|
| 无冠状动脉受累[n(%)] | 54(85.7) | 6(75.0) | χ2=0.07 | 0.787 |
| 冠状动脉扩张[n(%)] | 1(1.6) | 1(12.5) | - | 0.2141) |
| 冠状动脉瘤分型[n(%)] | ||||
| 小型 | 6(9.5) | 1(12.5) | - | 0.5841) |
| 中型 | 2(3.2) | 0(0.0) | - | 1.0001) |
| 巨大型 | 0(0.0) | 0(0.0) | - | - |
| 冠状动脉各分支Z值[M(P25~P75)] | ||||
| LM | 0.89(0.37~1.65) | 1.12(0.86~1.33) | Z=0.53 | 0.599 |
| LAD | 0.47(-0.03~1.06) | 0.51(0.30~0.89) | Z=0.25 | 0.799 |
| LCX | -0.12(-0.52~0.55) | -0.33(-0.64~-0.01) | Z=0.96 | 0.335 |
| RCA | 0.52(-0.16~0.91) | 0.11(-1.58~0.50) | Z=1.60 | 0.109 |
| [1] | Jone PN, Tremoulet A, Choueiter N, et al. Update on diagnosis and management of Kawasaki disease: a scientific statement from the american heart association[J]. Circulation, 2024, 150(23): e481-e500. |
| [2] |
Peng Y, Liu X, Duan Z, et al. Prevalence and characteristics of arthritis in Kawasaki disease: a Chinese cohort study[J]. Clin Exp Med, 2019, 19(2): 167-172.
doi: 10.1007/s10238-019-00547-w pmid: 30725203 |
| [3] |
Yasin S, Schulert GS. Systemic juvenile idiopathic arthritis and macrophage activation syndrome: update on pathogenesis and treatment[J]. Curr Opin Rheumatol, 2018, 30(5): 514-520.
doi: 10.1097/BOR.0000000000000526 pmid: 29870499 |
| [4] |
Nigrovic PA. Macrophage activation syndrome[J]. Arthritis Rheumatol, 2025, 77(4): 367-379.
doi: 10.1002/art.v77.4 |
| [5] | 吴建强, 沈丹萍, 卢美萍. 全身型幼年特发性关节炎相关难治性巨噬细胞活化综合征的挽救治疗1例报告[J]. 临床儿科杂志, 2025, 43(3): 216-219. |
| Wu JQ, Shen DP, Lu MP. Salvage therapy for refractory macrophage activation syndrome associated with systemic juvenile idiopathic arthritis: a case report[J]. Linchuang Erke Zazhi, 2025, 43(3): 216-219. | |
| [6] |
Ravelli A, Minoia F, Davì S, et al. 2016 Classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: a European league against rheumatism/american college of rheumatology/paediatric rheumatology international trials organisation collaborative initiative[J]. Arthritis Rheumatol, 2016, 68(3): 566-576.
doi: 10.1002/art.v68.3 |
| [7] |
Go E, van Veenendaal M, Manlhiot C, et al. Kawasaki disease and systemic juvenile idiopathic arthritis - two ends of the same spectrum[J]. Front Pediatr, 2021, 9: 665815.
doi: 10.3389/fped.2021.665815 |
| [8] |
Dogra S, Gehlot A, Suri D, et al. Incomplete Kawasaki disease followed by systemic onset juvenile idiopathic arthritis- the diagnostic dilemma[J]. Indian J Pediatr, 2013, 80(9): 783-785.
doi: 10.1007/s12098-012-0893-7 pmid: 23054859 |
| [9] |
Rigante D, Valentini P, Onesimo R, et al. Incomplete Kawasaki syndrome followed by systemic onset-juvenile idiopathic arthritis mimicking Kawasaki syndrome[J]. Rheumatol Int, 2010, 30(4): 535-539.
doi: 10.1007/s00296-009-0960-1 pmid: 19455336 |
| [10] | 翁慧沥, 白春然, 刘莹. 以川崎病起病的全身型幼年特发性关节炎1例[J]. 儿科药学杂志, 2025, 31(6): 61-63. |
| Weng HL, Bai CR, Liu Y. One case of systemic juvenile idiopathic arthritis onset with Kawasaki disease[J]. Erke Yaoxue Zazhi, 2025, 31(6): 61-63. | |
| [11] | McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American heart association[J]. Circulation, 2017, 135(17): e927-e999. |
| [12] | 金玉子, 陆菲. 幼年特发性关节炎全身型误诊16例分析[J]. 中国现代医生, 2009, 47(15): 216-217. |
| Jin YZ, Lu F. Analysis of 16 cases of misdiagnosis of systemic juvenile idiopathic arthritis[J]. Zhongguo Xiandai Yisheng, 2009, 47 (15): 216-217. | |
| [13] |
Martins A, Conde M, Brito M, et al. Arthritis in Kawasaki disease: a poorly recognised manifestation[J]. J Paediatr Child Health, 2018, 54(12): 1371-1374.
doi: 10.1111/jpc.2018.54.issue-12 |
| [14] |
Guleria S, Pilania RK, Jindal AK, et al. Clinico-laboratory profile of Kawasaki disease with arthritis in children[J]. Eur J Pediatr, 2020, 179(6): 875-879.
doi: 10.1007/s00431-020-03582-y pmid: 31974671 |
| [15] |
Kobayashi T, Inoue Y, Takeuchi K, et al. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease[J]. Circulation, 2006, 113(22): 2606-2612.
doi: 10.1161/CIRCULATIONAHA.105.592865 pmid: 16735679 |
| [16] |
Kim SH. Diagnosis of coronary artery abnormalities in Kawasaki disease: recent guidelines and z score systems[J]. Clin Exp Pediatr, 2022, 65(9): 430-438.
doi: 10.3345/cep.2021.01459 |
| [17] |
Petty RE, Southwood TR, Manners P, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001[J]. J Rheumatol, 2004, 31(2): 390-392.
pmid: 14760812 |
| [18] |
Martini A, Ravelli A, Avcin T, et al. Toward new classification criteria for juvenile idiopathic arthritis: first steps, pediatric rheumatology international trials organization international consensus[J]. J Rheumatol, 2019, 46(2): 190-197.
doi: 10.3899/jrheum.180168 pmid: 30275259 |
| [19] |
Kanemasa H, Nanishi E, Takada H, et al. Overlapping features in Kawasaki disease-related arthritis and systemic-onset juvenile idiopathic arthritis: a nationwide study in Japan[J]. Front Pediatr, 2021, 9: 597458.
doi: 10.3389/fped.2021.597458 |
| [20] | Wang D, Luo C, Tang XM, et al. Clinical analysis of systemic juvenile idiopathic arthritis with Kawasaki disease-like symptoms[J]. Zhonghua Erke Zazhi, 2024, 62(12): 1158-1163. |
| [21] |
Kumar S, Vaidyanathan B, Gayathri S, et al. Systemic onset juvenile idiopathic arthritis with macrophage activation syndrome misdiagnosed as Kawasaki disease: case report and literature review[J]. Rheumatol Int, 2013, 33(4): 1065-1069.
doi: 10.1007/s00296-010-1650-8 pmid: 21132551 |
| [22] |
Simonds MM, Brescia AC. Pathogenesis of juvenile idiopathic arthritis[J]. Curr Opin Rheumatol, 2025, 37(5): 321-326.
doi: 10.1097/BOR.0000000000001099 pmid: 40326416 |
| [23] |
Bordea MA, Costache C, Grama A, et al. Cytokine cascade in Kawasaki disease versus Kawasaki-like syndrome[J]. Physiol Res, 2022, 71(1): 17-27.
pmid: 35043641 |
| [24] |
Hattori S, Nozawa T, Nishimura K, et al. Characteristics of persistent arthritis with refractory Kawasaki disease: a single-center retrospective study[J]. Sci Rep, 2023, 13(1): 9890.
doi: 10.1038/s41598-023-36308-9 pmid: 37336934 |
| [25] |
Binstadt BA, Levine JC, Nigrovic PA, et al. Coronary artery dilation among patients presenting with systemic-onset juvenile idiopathic arthritis[J]. Pediatrics, 2005, 116(1): e89-e93.
doi: 10.1542/peds.2004-2190 pmid: 15930186 |
| [26] |
McCrindle BW, Harris KC. Coronary artery aneurysms after Kawasaki Disease: understanding the pathology[J]. Can J Cardiol, 2018, 34(9): 1094-1097.
doi: S0828-282X(18)30930-9 pmid: 30170663 |
| [27] | Aviña-Zubieta JA, Choi HK, Sadatsafavi M, et al. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies[J]. Arthritis Rheum, 2008, 59(12): 1690-1697. |
| [28] |
Zhang L, Wei Y, Zeng N, et al. A rare case of coronary artery complication in a child with systemic juvenile idiopathic arthritis and macrophage activation syndrome: case report and literature review[J]. Pediatr Rheumatol Online J, 2024, 22(1): 4.
doi: 10.1186/s12969-023-00944-2 pmid: 38166957 |
| [29] | 崔宁迅, 陈如月, 林强, 等. 以川崎病起病的全身型幼年特发性关节炎3例[J]. 江苏医药, 2021, 47(12): 1291-1295. |
| Cui NX, Chen RY, Lin Q, et al. Three cases of systemic juvenile idiopathic arthritis onset with Kawasaki disease[J]. Jiangsu Yiyao, 2021, 47(12): 1291-1295. | |
| [30] |
Dong S, Bout-Tabaku S, Texter K, et al. Diagnosis of systemic-onset juvenile idiopathic arthritis after treatment for presumed Kawasaki disease[J]. J Pediatr, 2015, 166(5): 1283-1288.
doi: 10.1016/j.jpeds.2015.02.003 |
| [31] |
Ae R, Makino N, Kosami K, et al. Epidemiology, treatments, and cardiac complications in patients with Kawasaki disease: the nationwide survey in Japan, 2017-2018[J]. J Pediatr, 2020, 225: 23-29.e2.
doi: 10.1016/j.jpeds.2020.05.034 |
| [32] | 邹丽霞, 卢美萍, 郭莉, 等. 托珠单抗治疗不完全川崎病伴有全身型幼年特发性关节炎一例[J]. 中华急诊医学杂志, 2017, 26(6): 715-716. |
| Zou LX, Lu MP, Guo L, et al. Tocilizumab in the treatment of one case of incomplete Kawasaki disease with systemic juvenile idiopathic arthritis[J]. Zhonghua Jizhen Yixue Zazhi, 2017, 26 (6): 715-716. |
| [1] | Rachel Rosen, Osvaldo Borrelli, Christophe Faure, Katja Karrento, Usha Krishnan, Samuel Nurko, Nathalie Rommel, Alan Silverman, Michiel van Wijk, Marc Benninga (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: upper gastrointestinal disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 595-608. |
| [2] | Carlo Di Lorenzo, Miguel Saps, Bruno P. Chumpitazi, Shaman Rajindrajith, Annamaria Staiano, Nikhil Thapar, Miranda van Tilburg, Carlos Velasco-Benítez, Arine Vlieger (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: lower and biliary disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 609-621. |
| [3] | LI Xufeng, TANG Haoxun, LI Xingjun, ZHANG Lize, GAO Chenqing, ZHAO Shunying, LIU Jianhua. Clinical characteristics, chest CT imaging phenotypes, and their correlation with prognosis in 76 children with Chlamydia pneumoniae pneumonia [J]. Journal of Clinical Pediatrics, 2026, 44(7): 622-627. |
| [4] | WANG Zhen, SHAO Jingbo, ZHANG Na, XIA Min, ZHU Jiashi, DU Chengkan, LI Hong. Factors influencing long-term recurrence in pediatric acute lymphoblastic leukemia patients with low-risk disease at initial diagnosis: a five-year follow-up analysis of 254 cases from a single center [J]. Journal of Clinical Pediatrics, 2026, 44(7): 628-635. |
| [5] | GUO Xuemei, XUE Yao, WANG Yongren, RONG Liucheng, FANG Yongjun, LIN Rufeng. Clinical features and prognosis of childhood acute myeloid leukemia with CBFA2T3::GLIS2 fusion [J]. Journal of Clinical Pediatrics, 2026, 44(7): 636-643. |
| [6] | YANG Lijun, FU Dongxia, CUI Yan, YANG Junmei, ZHANG Liming. Clinical manifestation and genetic analysis of CHARGE syndrome caused by CHD7 gene variation [J]. Journal of Clinical Pediatrics, 2026, 44(7): 644-650. |
| [7] | HU Yan, YANG Fan, LIANG Aimin, MAO Meng. Identification and management of faltering growth in children: insights from the 13th International Conference on Nutrition and Growth [J]. Journal of Clinical Pediatrics, 2026, 44(6): 485-488. |
| [8] | LI Jian, LI Tao, HE Lulu, WU Lei, HU Tianjiao, HUANG Yixuan, LIN Xinrong, SHEN Qiyang, PAN Sirui, XIE Nan, ZHOU Jianfeng, ZHOU Chunlei, ZHOU Li. A retrospective analysis of 50 cases of malignant rhabdoid tumor in children: clinical features, treatment response and prognostic factors [J]. Journal of Clinical Pediatrics, 2026, 44(6): 499-507. |
| [9] | LI Yanhua, ZHANG Huanhuan, YANG Jingwei, LIAO Xuelian, SHAO Jingbo, JIAO Yangyang, ZHANG Ting, HUANG Can, JIANG Shayi. Analysis of survival prognosis and related risk factors of pediatric head and neck rhabdomyosarcoma [J]. Journal of Clinical Pediatrics, 2026, 44(6): 518-523. |
| [10] | SHI Yongyuan, YANG Lijuan, LEI Wenting, XIONG Yurong, PAN Shujing, LI Yuelin, ZHANG Jiali, TIAN Maoqiang. Clinical characteristics and prognosis analysis of autoimmune encephalitis with movement disorders in children: A single-center retrospective study [J]. Journal of Clinical Pediatrics, 2026, 44(6): 532-539. |
| [11] | GU Xinjia, ZHENG Zhihui, MEI Lingli, ZHENG Jinxin, LIU Taixiang, ZHU Jihua. Burden of urinary system diseases in children and adolescents in China, 1990-2023 [J]. Journal of Clinical Pediatrics, 2026, 44(6): 546-555. |
| [12] | CHEN Xumei, AIERKEN Aibibai, YUE Xueyan, RU Liang, ZHANG Li. A study on the latent profile analysis of psychological resilience and coping styles of parents of children with asthma and its influencing factors [J]. Journal of Clinical Pediatrics, 2026, 44(6): 556-563. |
| [13] | LUO Zihao, LI Shaojun, REN Peizhen, WANG Yanhong, GENG Gang. Analysis of clinical characteristics of children with pneumonia complicated with plastic bronchitis and establishment and validation of risk prediction model [J]. Journal of Clinical Pediatrics, 2026, 44(6): 564-572. |
| [14] | CHU Weihong, XU Liyan, PENG Shao, LAI Jianming. Lower extremity arterial thrombosis as first clinical manifestation in children's systemic lupus erythematosus complicated with antiphospholipid syndrome: a two-case report [J]. Journal of Clinical Pediatrics, 2026, 44(6): 579-583. |
| [15] | CHEN Liuwang, LIU Pan, XI Rongjuan, ZHANG Xianxia, ZHANG Yi, WEI Xingjiao, SU Min, YANG Yonghong, FU Yangxi. Methylmalonic acidemia with homocystinemia causing subacute combined degeneration of the spinal cord : a case report [J]. Journal of Clinical Pediatrics, 2026, 44(6): 584-588. |
|
||