

Journal of Clinical Pediatrics ›› 2026, Vol. 44 ›› Issue (7): 628-635.doi: 10.12372/jcp.2026.25e0888
• Clinical Research • Previous Articles Next Articles
WANG Zhen1, SHAO Jingbo1, ZHANG Na1, XIA Min2, ZHU Jiashi1, DU Chengkan2, LI Hong1( )
)
Received:2025-07-23
Revised:2025-11-04
Accepted:2025-11-26
Published:2026-07-15
Online:2026-07-12
Contact:
LI Hong
E-mail:lihonglily1978@sina.com
CLC Number:
WANG Zhen, SHAO Jingbo, ZHANG Na, XIA Min, ZHU Jiashi, DU Chengkan, LI Hong. Factors influencing long-term recurrence in pediatric acute lymphoblastic leukemia patients with low-risk disease at initial diagnosis: a five-year follow-up analysis of 254 cases from a single center[J].Journal of Clinical Pediatrics, 2026, 44(7): 628-635.
Table 1
Kaplan-Meier analysis of prognostic factors for survival in children with newly diagnosed low risk ALL"
| 项 目 | 例数(%) | RFS率( $\bar{x}±E$)/% | χ2值 | P | OS率( $\bar{x}±E$)/% | χ2值 | P |
|---|---|---|---|---|---|---|---|
| 性别 | 2.07 | 0.150 | 0.14 | 0.700 | |||
| 男 | 138(54.3) | 83.7±3.2 | 94.1±2.0 | ||||
| 女 | 116(45.7) | 88.8±3.3 | 92.2±2.8 | ||||
| 年龄 | 0.32 | 0.571 | 0.80 | 0.370 | |||
| <3岁 | 200(78.7) | 87.2±2.4 | 92.3±2.0 | ||||
| ≥3岁 | 54(21.3) | 87.0±5.2 | 96.3±2.6 | ||||
| 初诊WBC计数 | 0.67 | 0.411 | 0.31 | 0.576 | |||
| <30×109/L | 249(98.0) | 88.1±2.1 | 93.1±1.7 | ||||
| ≥30×109/L | 5(2.0) | 100 | 100 | ||||
| 初诊血红蛋白 | 0.54 | 0.460 | 0.17 | 0.673 | |||
| <100 g/L | 213(83.8) | 87.4±2.3 | 92.8±1.9 | ||||
| ≥100 g/L | 41(16.2) | 90.2±4.6 | 95.1±3.4 | ||||
| 初诊血小板计数 | 2.63 | 0.104 | 2.23 | 0.135 | |||
| <100×109/L | 162(63.7) | 84.7±2.9 | 91.2±2.4 | ||||
| ≥100×109/L | 92(36.3) | 90.1±3.4 | 96.7±1.9 | ||||
| 免疫分型 | 1.47 | 0.478 | 2.33 | 0.311 | |||
| Pro-B | 2(0.8) | 100.0 | 100.0 | ||||
| Common-B | 209(82.2) | 88.8±2.2 | 94.6±1.6 | ||||
| Pre-B | 43(17.0) | 80.4±6.2 | 87.1±5.5 | ||||
| Pred/Dex早期治疗反应 | 0.34 | 0.560 | 1.34 | 0.246 | |||
| 好 | 91(57.5) | 88.3±2.7 | 92.0±3.4 | ||||
| 不佳 | 67(42.5) | 84.4±3.7 | 87.8±4.1 | ||||
| 治疗方案 | 0.14 | 0.708 | 3.43 | 0.064 | |||
| 2009方案 | 111(43.7) | 85.2±3.4 | 90.1±2.8 | ||||
| 2015方案 | 143(56.3) | 87.6±2.8 | 96.5±1.5 | ||||
| 第19天骨髓是否缓解 | 8.53 | 0.003 | 18.94 | <0.001 | |||
| 缓解 | 247(97.2) | 89.2±2.0 | 94.2±1.6 | ||||
| 未缓解 | 7(2.8) | 57.1±18.7 | 57.1±18.7 | ||||
| D19 MRD | 4.06 | 0.044 | 10.11 | 0.001 | |||
| <1.0% | 230(90.6) | 89.3±2.1 | 95.6±1.4 | ||||
| ≥1.0% | 24(9.4) | 73.9±9.3 | 79.2±8.3 | ||||
| 巩固后MRD | 6.07 | 0.014 | 16.15 | <0.001 | |||
| <0.01% | 224(88.1) | 89.4±2.1 | 95.9±1.3 | ||||
| ≥0.01% | 30(11.9) | 72.3±8.3 | 75.6±8.1 | ||||
| TEL/AML1融合基因 | 0.03 | 0.845 | 0.31 | 0.576 | |||
| 阳性 | 80(31.4) | 84.8±4.7 | 93.4±3.5 | ||||
| 阴性 | 174(68.6) | 86.4±2.6 | 93.0±1.9 | ||||
| 高二倍体 | 2.02 | 0.155 | 0.12 | 0.721 | |||
| 是 | 41(16.1) | 79.2±6.6 | 92.7±4.1 | ||||
| 否 | 213(83.9) | 89.5±2.1 | 93.4±1.8 | ||||
| CNS状态 | 0.75 | 0.686 | 2.26 | 0.323 | |||
| 正常 | 247(97.2) | 87.6±2.1 | 93.9±1.5 | ||||
| CNS2 | 4(1.5) | 50.0±35.4 | 50.0±35.4 | ||||
| 损伤 | 3(1.3) | 100 | 100 |
Figure 1
10-year survival curves in children with newly diagnosed low risk ALL"
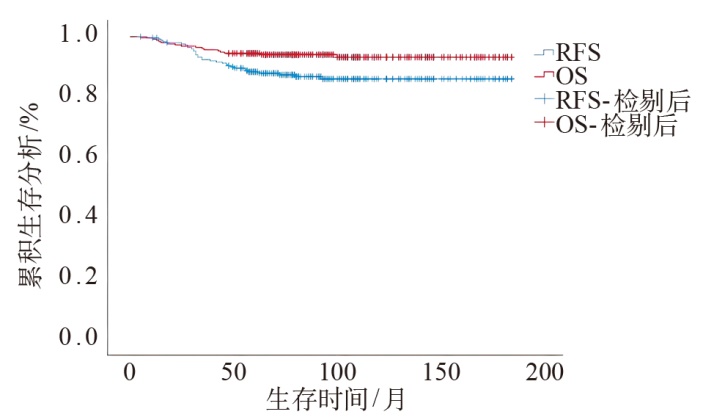
Figure 2
RFS survival curves of different post-consolidation MRD status in children with newly diagnosed low risk ALL"
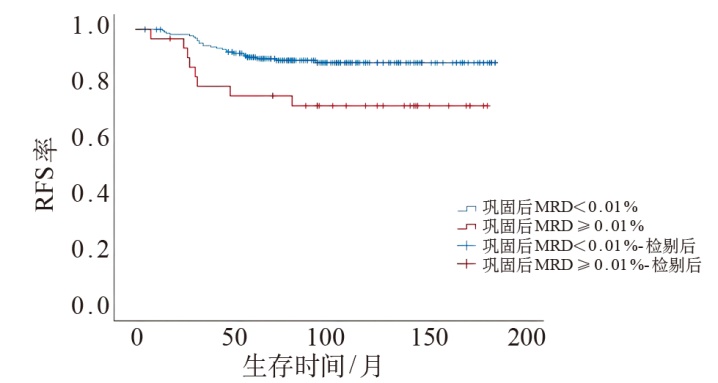
Table 2
Clinical features and group comparison in newly diagnosed low-risk ALL children"
| 项 目 | 例数(n) | 2009方案组例数[n/%] | 2015方案组例数[n/%] | χ2值 | P |
|---|---|---|---|---|---|
| 性别 | 0.03 | 0.860 | |||
| 男 | 138 | 61(44.2) | 77(55.8) | ||
| 女 | 116 | 50(43.1) | 66(56.9) | ||
| 年龄 | 0.01 | 0.901 | |||
| <3岁 | 200 | 87(43.5) | 113(56.6) | ||
| ≥3岁 | 54 | 24(44.4) | 30(55.6) | ||
| 初诊白细胞计数 | 1.16 | 0.281 | |||
| <30×109/L | 249 | 110(44.2) | 139(55.8) | ||
| ≥30×109/L | 5 | 1(20.0) | 4(80.0) | ||
| TEL/AML1融合基因 | 0.08 | 0.777 | |||
| 阳性 | 80 | 36(45.0) | 44(55.0) | ||
| 阴性 | 174 | 75(43.1) | 99(56.9) | ||
| 高二倍体 | 2.85 | 0.091 | |||
| 是 | 41 | 13(31.7) | 28(68.3) | ||
| 否 | 213 | 98(46.0) | 115(54.0) |
Table 3
Cox multivariate regression analysis of prognostic factors for RFS in children with newly diagnosed low risk ALL"
| 因 素 | β | SE | Wald χ2 | HR | 95%CI | P |
|---|---|---|---|---|---|---|
| 第19天骨髓是否缓解 | ||||||
| 缓解 | 1 | |||||
| 未缓解 | 1.180 | 0.673 | 3.071 | 3.253 | 0.870~12.171 | 0.080 |
| D19 MRD | ||||||
| <0.1% | 1 | |||||
| ≥1.0% | 0.416 | 0.519 | 0.642 | 1.516 | 0.548~4.192 | 0.432 |
| 巩固后MRD | ||||||
| <0.01% | 1 | |||||
| ≥0.01% | 0.854 | 0.415 | 4.223 | 2.348 | 1.040~5.300 | 0.040 |
| [1] | Angiolillo AL, Schore RJ, Kairalla JA, et al. Excellent outcomes with reduced frequency of vincristine and dexamethasone pulses in standard-risk B-lymphoblastic leukemia:results from Children's Oncology Group AALL0932[J/OL]. J Clin Oncol, 2021, 39(13): 1437-1447. https://doi.org/10.1200/JCO.20.00494. |
| [2] | Mattano LA Jr, Devidas M, Maloney KW, et al. Favorable trisomies and ETV6-RUNX1 predict cure in low-risk B-Cell acute lymphoblastic leukemia: results from Children's Oncology Group Trial AALL0331[J/OL]. J Clin Oncol, 2021, 39(14): 1540-1552. https://doi.org/10.1200/JCO.20.00494. |
| [3] | Campbell M, Kiss C, Zimmermann M, et al. Childhood acute lymphoblastic leukemia:results of the randomized acute lymphoblastic leukemia intercontinental-Berlin-Frankfurt-Munster 2009 trial[J/OL]. J Clin Oncol, 2023, 41(19): 3499-3511. https://doi.org/10.1200/JCO.22.01760. |
| [4] | 中华医学会儿科学分会血液学组, 中华儿科杂志编辑委员会. 儿童急性淋巴细胞白血病诊疗建议(第三次修订草案)[J/OL]. 中华儿科杂志, 2006, 44(5): 392-395. https://doi.org/10.3760/j.issn:0578-1310.2006.05.023. |
| The Subspecialty Group of Hematology, the Society of Pediatrics, Chinese Medical Association, the Editorial Board, Chinese Journal of Pediatrics. Suggestion of diagnosis and treatment of acute lymphoblastic leukemia in childhood (the 3rd revised version)[J/OL]. Zhonghua Erke Zazhi, 2006, 44( 5): 392-395. https://doi.org/10.3760/j.issn:0578-1310.2006.05.023. | |
| [5] | Liu K, Chu J, Dai Y, et al. Long-term follow-up of acute lymphoblastic leukemia in young children treated by the SCMC-ALL-2009 protocol[J/OL]. Leuk Lymphoma, 2020, 61(12): 2850-2858. https://doi.org/10.1080/10428194.2020.1786557. |
| [6] | Chinese Children's Cancer Group Acute Lymphoblastic Leukemia Study. Report of Chinese Children's Cancer Group acute lymphoblastic leukemia 2015 multicenter study[J/OL]. Zhonghua Erke Zazhi, 2022, 60(10): 1002-1010. https://doi.org/10.3760/cma.j.cn112140-20220719-00895. |
| [7] | Zhuang Y, Wu K, Zhu X, et al. Reduced dose intensity of daunorubicin during remission induction for low-risk patients with acute lymphoblastic leukemia: a retrospective cohort study of the Chinese Children's Cancer Group[J/OL]. Front Oncol, 2022, 12: 911567. https://doi.org/10.3389/fonc.2022.911567. |
| [8] | Omar AA, Basiouny L, Elnoby S, et al. St. St. Jude Total Therapy studies from I to XVII for childhood acute lymphoblastic leukemia:a brief review[J/OL]. J Egypt Natl Canc Inst, 2022, 34(1): 25. https://doi.org/10.1186/s43046-022-00126-3. |
| [9] | Chen X, Yu J. Survival and prognostic factors for relapsed childhood acute lymphoblastic leukemia after treatment with the Chinese children's cancer group ALL-2015 protocol:a single center results[J/OL]. Front Oncol, 2024, 14: 1405347. https://doi.org/10.3389/fonc.2024. |
| [10] | Chang TC, Chen W, Qu C, et al. Genomic determinants of outcome in acute lymphoblastic leukemia[J/OL]. J Clin Oncol, 2024, 42(29): 3491-3503. https://doi.org/10.1200/JCO.23.02238. |
| [11] | Tang J, Yu J, Cai J, et al. Prognostic factors for CNS control in children with acute lymphoblastic leukemia treated without cranial irradiation[J/OL]. Blood, 2021, 138(4): 331-343. https://doi.org/10.1182/blood.2020010438. |
| [12] | Place AE, Stevenson KE, Vrooman LM, et al. Intravenous pegylated asparaginase versus intramuscular native Escherichia coli L-asparaginase in newly diagnosed childhood acute lymphoblastic leukaemia (DFCI 05-001): a randomised, open-label phase 3 trial[J/OL]. Lancet Oncol, 2015, 16(16): 1677-1690. https://doi.org/10.1016/S1470-2045(15)00363-0. |
| [13] | Yu CH, Jou ST, Su H, et al. Clinical impact of minimal residual disease and genetic subtypes on the prognosis of childhood acute lymphoblastic leukemia[J/OL]. Cancer, 2023, 129(5): 790-802. https://doi.org/10.1002/cncr.34606. |
| [14] | Huang XT, Wang CJ, Gao C, et al. Relationship between subtype-specific minimal residual disease level and long-term prognosis in children with acute lymphoblastic leukemia[J/OL]. Ann Hematol, 2024, 103(9): 3657-3665. https://doi.org/10.1007/s00277-024-05687-y. |
| [15] | Popov A, Henze G, Roumiantseva J, et al. Flow cytometric MRD at the end of consolidation in childhood B-lineage acute lymphoblastic leukemia has significant prognostic value but limited clinical implications:results of study ALL-MB 2008[J/OL]. Leuk Res, 2023, 125: 106998. https://doi.org/10.1016/j.leukres.2022.106998. |
| [16] | Gupta S, Rau RE, Kairalla JA, et al. Blinatumomab in standard-risk B-cell acute lymphoblastic leukemia in children[J/OL]. N Engl J Med, 2025, 392(9): 875-891. https://doi.org/10.1056/NEJMoa2411680. |
| [17] | Svaton M, Skotnicova A, Reznickova L, et al. NGS better discriminates true MRD positivity for the risk stratification of childhood ALL treated on an MRD-based protocol[J/OL]. Blood, 2023, 141(5): 529-533. https://doi.org/10.1182/blood.2022017003. |
| [18] | Rheingold SR, Bhojwani D, Ji L, et al. Determinants of survival after first relapse of acute lymphoblastic leukemia: a Children’s Oncology Group study[J/OL]. Leukemia, 2024, 38(11): 2382-2394. https://doi.org/10.1038/s41375-024-02395-4. |
| [19] | Hogan LE, Bhatla T, Xu X, et al. Severe toxicity and poor efficacy of reinduction chemotherapy are associated with overall poor outcomes in relapsed B-cell acute lymphoblastic leukemia:a report from the Children's Oncology Group AALL1331 trial[J/OL]. Haematologica, 2025, 110(12): 2930-2941. https://doi.org/10.3324/haematol.2025.287386. |
| [1] | Rachel Rosen, Osvaldo Borrelli, Christophe Faure, Katja Karrento, Usha Krishnan, Samuel Nurko, Nathalie Rommel, Alan Silverman, Michiel van Wijk, Marc Benninga (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: upper gastrointestinal disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 595-608. |
| [2] | Carlo Di Lorenzo, Miguel Saps, Bruno P. Chumpitazi, Shaman Rajindrajith, Annamaria Staiano, Nikhil Thapar, Miranda van Tilburg, Carlos Velasco-Benítez, Arine Vlieger (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: lower and biliary disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 609-621. |
| [3] | LI Xufeng, TANG Haoxun, LI Xingjun, ZHANG Lize, GAO Chenqing, ZHAO Shunying, LIU Jianhua. Clinical characteristics, chest CT imaging phenotypes, and their correlation with prognosis in 76 children with Chlamydia pneumoniae pneumonia [J]. Journal of Clinical Pediatrics, 2026, 44(7): 622-627. |
| [4] | GUO Xuemei, XUE Yao, WANG Yongren, RONG Liucheng, FANG Yongjun, LIN Rufeng. Clinical features and prognosis of childhood acute myeloid leukemia with CBFA2T3::GLIS2 fusion [J]. Journal of Clinical Pediatrics, 2026, 44(7): 636-643. |
| [5] | YANG Lijun, FU Dongxia, CUI Yan, YANG Junmei, ZHANG Liming. Clinical manifestation and genetic analysis of CHARGE syndrome caused by CHD7 gene variation [J]. Journal of Clinical Pediatrics, 2026, 44(7): 644-650. |
| [6] | HU Yan, YANG Fan, LIANG Aimin, MAO Meng. Identification and management of faltering growth in children: insights from the 13th International Conference on Nutrition and Growth [J]. Journal of Clinical Pediatrics, 2026, 44(6): 485-488. |
| [7] | LIU Ziyao, WANG Congying, WANG Hongmao, ZHANG Mingming, XU Yingjie, LAI Jianming, NIU Wenquan, LI Xiaohui. Early differentiation of Kawasaki disease with joint symptoms and systemic juvenile idiopathic arthritis with Kawasaki disease-like symptoms: a single-center retrospective study [J]. Journal of Clinical Pediatrics, 2026, 44(6): 489-498. |
| [8] | LI Jian, LI Tao, HE Lulu, WU Lei, HU Tianjiao, HUANG Yixuan, LIN Xinrong, SHEN Qiyang, PAN Sirui, XIE Nan, ZHOU Jianfeng, ZHOU Chunlei, ZHOU Li. A retrospective analysis of 50 cases of malignant rhabdoid tumor in children: clinical features, treatment response and prognostic factors [J]. Journal of Clinical Pediatrics, 2026, 44(6): 499-507. |
| [9] | LI Yue, XIE Zhiwei, TANG Yanjing, LI Benshang. A comparative study on the efficacy of two CD19/CD22 dual-targeting CAR-T strategies in children with relapsed/refractory B-cell acute lymphoblastic leukemia with PAX5 gene variations [J]. Journal of Clinical Pediatrics, 2026, 44(6): 508-517. |
| [10] | LI Yanhua, ZHANG Huanhuan, YANG Jingwei, LIAO Xuelian, SHAO Jingbo, JIAO Yangyang, ZHANG Ting, HUANG Can, JIANG Shayi. Analysis of survival prognosis and related risk factors of pediatric head and neck rhabdomyosarcoma [J]. Journal of Clinical Pediatrics, 2026, 44(6): 518-523. |
| [11] | SHI Yongyuan, YANG Lijuan, LEI Wenting, XIONG Yurong, PAN Shujing, LI Yuelin, ZHANG Jiali, TIAN Maoqiang. Clinical characteristics and prognosis analysis of autoimmune encephalitis with movement disorders in children: A single-center retrospective study [J]. Journal of Clinical Pediatrics, 2026, 44(6): 532-539. |
| [12] | GU Xinjia, ZHENG Zhihui, MEI Lingli, ZHENG Jinxin, LIU Taixiang, ZHU Jihua. Burden of urinary system diseases in children and adolescents in China, 1990-2023 [J]. Journal of Clinical Pediatrics, 2026, 44(6): 546-555. |
| [13] | CHEN Xumei, AIERKEN Aibibai, YUE Xueyan, RU Liang, ZHANG Li. A study on the latent profile analysis of psychological resilience and coping styles of parents of children with asthma and its influencing factors [J]. Journal of Clinical Pediatrics, 2026, 44(6): 556-563. |
| [14] | LUO Zihao, LI Shaojun, REN Peizhen, WANG Yanhong, GENG Gang. Analysis of clinical characteristics of children with pneumonia complicated with plastic bronchitis and establishment and validation of risk prediction model [J]. Journal of Clinical Pediatrics, 2026, 44(6): 564-572. |
| [15] | CHU Weihong, XU Liyan, PENG Shao, LAI Jianming. Lower extremity arterial thrombosis as first clinical manifestation in children's systemic lupus erythematosus complicated with antiphospholipid syndrome: a two-case report [J]. Journal of Clinical Pediatrics, 2026, 44(6): 579-583. |
|
||