

Journal of Clinical Pediatrics ›› 2026, Vol. 44 ›› Issue (6): 499-507.doi: 10.12372/jcp.2026.25e1054
• Original Article • Previous Articles Next Articles
LI Jian1, LI Tao1, HE Lulu2, WU Lei1, HU Tianjiao3, HUANG Yixuan4, LIN Xinrong1, SHEN Qiyang1, PAN Sirui1, XIE Nan1, ZHOU Jianfeng1, ZHOU Chunlei5, ZHOU Li1( )
)
Received:2025-08-27
Revised:2026-02-06
Accepted:2026-02-11
Published:2026-06-15
Online:2026-06-04
Contact:
ZHOU Li
E-mail:zhoulinjey@163.com
CLC Number:
LI Jian, LI Tao, HE Lulu, WU Lei, HU Tianjiao, HUANG Yixuan, LIN Xinrong, SHEN Qiyang, PAN Sirui, XIE Nan, ZHOU Jianfeng, ZHOU Chunlei, ZHOU Li. A retrospective analysis of 50 cases of malignant rhabdoid tumor in children: clinical features, treatment response and prognostic factors[J].Journal of Clinical Pediatrics, 2026, 44(6): 499-507.
Table 1
Comparison of clinical characteristics among patients with MRT at three distinct anatomical sites"
| 项 目 | ATRT组(n=18) | MRTK组(n=17) | EERT组(n=15) | 统计量 | P |
|---|---|---|---|---|---|
| 发病年龄[M(P25~P75)]/月 | 33(26~55) | 24(8~33) | 19(14~52) | H=3.54 | 0.170 |
| 男性[n(%)] | 8(44.4) | 6(35.3) | 7(46.7) | χ2=0.49 | 0.782 |
| LDH[M(P25~P75)]/U·L-1 | 276(210~385) | 350(242~540) | 319(248~338) | H=1.79 | 0.408 |
| 完整手术切除[n(%)] | 13(72.2) | 13(76.5) | 8(53.3) | χ2=2.19 | 0.334 |
| 放疗[n(%)] | 14(77.8) | 7(41.2) | 6(40.0) | χ2=6.41 | 0.041 |
| 转移[n(%)] | 9(50.0) | 12(70.6) | 5(33.3) | χ2=4.48 | 0.107 |
| 死亡[n(%)] | 6(33.3) | 10(58.8) | 3(20.0) | χ2=5.36 | 0.069 |
Figure 1
Survival curve of 50 patients with MRT"
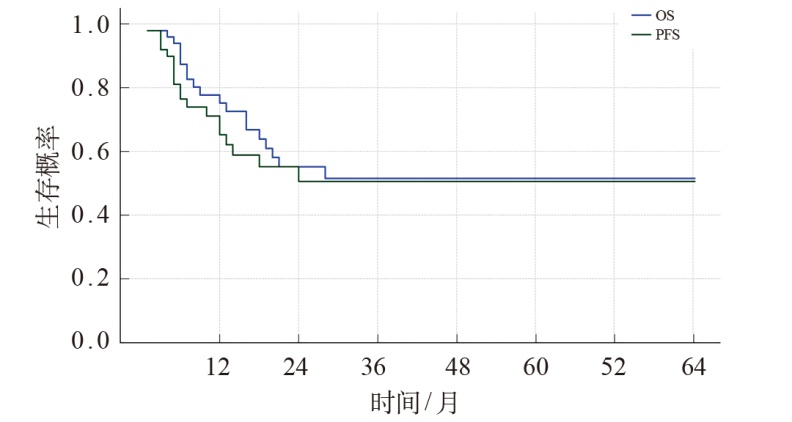
Table 2
Univariate and multivariate COX regression model analysis of OS in 50 children with MRT"
| 变 量 | 总例数 | 死亡例数 | 单因素分析 | 多因素分析 | ||||
|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |||
| 诊断年龄 | ||||||||
| ≥1岁(参考) | 39 | 13 | - | - | - | - | - | - |
| <1岁 | 11 | 6 | 2.99 | 1.11~8.07 | 0.030 | 1.07 | 0.29~3.98 | 0.918 |
| 性别 | ||||||||
| 男(参考) | 21 | 8 | - | - | - | |||
| 女 | 29 | 11 | 0.83 | 0.34~2.08 | 0.697 | |||
| 手术 | ||||||||
| 完整切除(参考) | 34 | 11 | - | - | - | - | - | - |
| 未完整切除 | 16 | 8 | 4.49 | 1.68~11.97 | 0.003 | 5.42 | 1.61~18.20 | 0.006 |
| LDH | ||||||||
| >345U/L(参考) | 15 | 10 | - | - | - | - | - | - |
| ≤345U/L | 35 | 9 | 0.19 | 0.08~0.49 | <0.001 | 0.16 | 0.05~0.48 | 0.001 |
| 放疗 | ||||||||
| 是(参考) | 27 | 8 | - | - | - | - | - | - |
| 否 | 23 | 11 | 2.87 | 1.14~7.22 | 0.025 | 1.57 | 0.45~5.45 | 0.476 |
| 转移 | ||||||||
| 是(参考) | 26 | 13 | - | - | - | - | - | - |
| 否 | 24 | 6 | 0.32 | 0.12~0.84 | 0.022 | 0.23 | 0.07~0.75 | 0.015 |
| [1] |
Beckwith JB, Palmer NF. Histopathology and prognosis of Wilms tumors: results from the First National Wilms' Tumor Study[J]. Cancer, 1978, 41(5): 1937-1948.
doi: 10.1002/1097-0142(197805)41:5<1937::aid-cncr2820410538>3.0.co;2-u pmid: 206343 |
| [2] |
Sultan I, Qaddoumi I, Rodríguez-Galindo C, et al. Age, stage, and radiotherapy, but not primary tumor site, affects the outcome of patients with malignant rhabdoid tumors[J]. Pediatr Blood Cancer, 2010, 54(1): 35-40.
doi: 10.1002/pbc.22285 pmid: 19798737 |
| [3] |
van den Heuvel-Eibrink MM, van Tinteren H, Rehorst H, et al. Malignant rhabdoid tumours of the kidney (MRTKs), registered on recent SIOP protocols from 1993 to 2005: a report of the SIOP renal tumour study group[J]. Pediatr Blood Cancer, 2011, 56(5): 733-737.
doi: 10.1002/pbc.22922 pmid: 21370404 |
| [4] |
Tomlinson GE, Breslow NE, Dome J, et al. Rhabdoid tumor of the kidney in the National Wilms' Tumor Study: age at diagnosis as a prognostic factor[J]. J Clin Oncol, 2005, 23(30): 7641-7645.
pmid: 16234525 |
| [5] |
Geller JI, Roth JJ, Biegel JA. Biology and treatment of rhabdoid tumor[J]. Crit Rev Oncog, 2015, 20(3-4): 199-216.
pmid: 26349416 |
| [6] |
Liu NQ, Paassen I, Custers L, et al. SMARCB1 loss activates patient-specific distal oncogenic enhancers in malignant rhabdoid tumors[J]. Nat Commun, 2023, 14(1): 7762.
doi: 10.1038/s41467-023-43498-3 |
| [7] |
Eaton KW, Tooke LS, Wainwright LM, et al. Spectrum of SMARCB1/INI1 mutations in familial and sporadic rhabdoid tumors[J]. Pediatr Blood Cancer, 2011, 56(1): 7-15.
doi: 10.1002/pbc.v56:1 |
| [8] |
Hoot AC, Russo P, Judkins AR, et al. Immunohistochemical analysis of hSNF5/INI1 distinguishes renal and extra-renal malignant rhabdoid tumors from other pediatric soft tissue tumors[J]. Am J Surg Pathol, 2004, 28(11): 1485-1491.
pmid: 15489652 |
| [9] | 封淑月, 张姮, 孙梦娇, 等. AVDC/ICE方案治疗10例儿童颅外恶性横纹肌样瘤的临床疗效分析[J]. 临床儿科杂志, 2024, 42(12): 1032-1038. |
| Feng SY, Zhang H, Sun MJ, et al. Clinical efficacy analysis of AVDC/ICE regimen in the treatment of 10 pediatric extracranial malignant rhabdoid tumors[J]. Linchuang Erke Zazhi, 2024, 42(12): 1032-1038. | |
| [10] |
Slavc I, Chocholous M, Leiss U, et al. Atypical teratoid rhabdoid tumor: improved long-term survival with an intensive multimodal therapy and delayed radiotherapy. The Medical University of Vienna Experience 1992-2012[J]. Cancer Med, 2014, 3(1): 91-100.
doi: 10.1002/cam4.2014.3.issue-1 |
| [11] |
Benesch M, Bartelheim K, Fleischhack G, et al. High-dose chemotherapy (HDCT) with auto-SCT in children with atypical teratoid/rhabdoid tumors (AT/RT): a report from the European Rhabdoid Registry (EU-RHAB)[J]. Bone Marrow Transplant, 2014, 49(3): 370-375.
doi: 10.1038/bmt.2013.208 |
| [12] | 李健, 李涛, 何璐璐, 等. 儿童颅外恶性横纹肌样瘤21例临床及预后分析[J]. 中华实用儿科临床杂志, 2024, 39(9): 683-687. |
| Li J, Li T, He LL, et al. Clinical and prognostic analysis of 21 cases of extracranial malignant rhabdoid tumors in children[J]. Zhonghua Shiyong Erke Linchuang Zazhi, 2024, 39(9): 683-687. | |
| [13] |
Daw NC, Chi YY, Kim Y, et al. Treatment of stage I anaplastic Wilms' tumour: a report from the Children's Oncology Group AREN0321 study[J]. Eur J Cancer, 2019, 118: 58-66.
doi: S0959-8049(19)30361-2 pmid: 31325873 |
| [14] | 周莉, 方拥军, 芮耀耀, 等. 儿童横纹肌肉瘤临床治疗评估[J]. 临床儿科杂志, 2018, 36(8): 584-586. |
| Zhou L, Fang YJ, Rui YY, et al. Evaluation of clinical treatment of rhabdomyosarcoma in children[J]. Linchuang Erke Zazhi, 2018, 36(8): 584-586. | |
| [15] |
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada[J]. J Natl Cancer Inst, 2000, 92(3): 205-216.
doi: 10.1093/jnci/92.3.205 pmid: 10655437 |
| [16] | 徐艳丽, 管文斌, 茅伟伟, 等. 52例颅内非典型畸胎样/横纹肌样瘤的临床特征及生存分析[J]. 上海交通大学学报(医学版), 2021, 41(9): 1222-1227. |
| Xu YL, Guan WB, Mao WW, et al. Clinical characteristics and survival analysis of 52 cases of intracranial atypical teratoid/rhabdoid tumors[J]. Shanghai Jiaotong Daxue Xuebao (Yixueban), 2021, 41(9): 1222-1227. | |
| [17] | Horazdovsky R, Manivel JC, Cheng EY. Surgery and actinomycin improve survival in malignant rhabdoid tumor[J]. Sarcoma, 2013, 2013: 315170. |
| [18] |
Han Y, Dong Y, Lian K, et al. Multidisciplinary management of pediatric malignant rhabdoid tumor based on 5 years of experience at a tertiary care center[J]. Pediatr Surg Int, 2022, 39(1): 51.
doi: 10.1007/s00383-022-05338-1 pmid: 36522484 |
| [19] | 成海燕, 杨深, 蔡思雨, 等. 35例儿童肾恶性横纹肌样瘤临床及预后特征[J]. 中国小儿血液与肿瘤杂志, 2018, 23(3): 118-123. |
| Cheng HY, Yang S, Cai SY, et al. Clinical and prognostic characteristics of 35 children with renal malignant rhabdoid tumor[J]. Zhongguo Xiaoer Xueye Yu Zhongliu Zazhi, 2018, 23(3): 118-123. | |
| [20] |
Frühwald MC, Hasselblatt M, Nemes K, et al. Age and DNA methylation subgroup as potential independent risk factors for treatment stratification in children with atypical teratoid/rhabdoid tumors[J]. Neuro Oncol, 2020, 22(7): 1006-1017.
doi: 10.1093/neuonc/noz244 |
| [21] |
Nemes K, Bens S, Kachanov D, et al. Clinical and genetic risk factors define two risk groups of extracranial malignant rhabdoid tumours (eMRT/RTK)[J]. Eur J Cancer, 2021, 142: 112-122.
doi: 10.1016/j.ejca.2020.10.004 pmid: 33249395 |
| [22] |
Alva E, Rubens J, Chi S, et al. Recent progress and novel approaches to treating atypical teratoid rhabdoid tumor[J]. Neoplasia, 2023, 37: 100880.
doi: 10.1016/j.neo.2023.100880 |
| [23] |
Xie S, Fang Y, Yang Y, et al. Extracranial malignant rhabdoid tumors in children: high mortality even with the help of an aggressive clinical approach[J]. Eur J Pediatr, 2024, 183(2): 557-567.
doi: 10.1007/s00431-023-05345-x |
| [24] |
Cheng H, Yang S, Cai S, et al. Clinical and prognostic characteristics of 53 cases of extracranial malignant rhabdoid tumor in children. A single-institute experience from 2007 to 2017[J]. Oncologist, 2019, 24(7): e551-e558.
doi: 10.1634/theoncologist.2018-0416 |
| [25] |
Fidani P, De Ioris MA, Serra A, et al. A multimodal strategy based on surgery, radiotherapy, ICE regimen and high dose chemotherapy in atypical teratoid/rhabdoid tumours: a single institution experience[J]. J Neurooncol, 2009, 92(2): 177-183.
doi: 10.1007/s11060-008-9750-y |
| [26] |
Reddy AT, Strother DR, Judkins AR, et al. Efficacy of high-dose chemotherapy and three-dimensional conformal radiation for atypical teratoid/rhabdoid tumor: a report from the children's oncology group trial ACNS0333[J]. J Clin Oncol, 2020, 38(11): 1175-1185.
doi: 10.1200/JCO.19.01776 pmid: 32105509 |
| [27] |
Brennan B, De Salvo GL, Orbach D, et al. Outcome of extracranial malignant rhabdoid tumours in children registered in the European Paediatric Soft Tissue Sarcoma Study Group Non-Rhabdomyosarcoma Soft Tissue Sarcoma 2005 Study-EpSSG NRSTS 2005[J]. Eur J Cancer, 2016, 60: 69-82.
doi: 10.1016/j.ejca.2016.02.027 pmid: 27082136 |
| [28] | 刘红艳, 刘琦, 张迎丽, 等. 自体造血干细胞移植治疗儿童非典型畸胎瘤样/横纹肌样瘤[J]. 中国小儿血液与肿瘤杂志, 2023, 28(3): 186-190. |
| Liu HY, Liu Q, Zhang YL, et al. Autologous hematopoietic stem cell transplantation for the treatment of atypical teratoid/rhabdoid tumors in children[J]. Zhongguo Xiaoer Xueye Yu Zhongliu Zazhi, 2023, 28(3): 186-190. | |
| [29] | Furtwängler R, Kager L, Melchior P, et al. High-dose treatment for malignant rhabdoid tumor of the kidney: no evidence for improved survival-The Gesellschaft für Pädiatrische Onkologie und Hämatologie (GPOH) experience[J]. Pediatr Blood Cancer, 2018, 65(1). doi: 10.1002/pbc.26746. |
| [30] |
Bourdeaut F, Lequin D, Brugières L, et al. Frequent hSNF5/INI1 germline mutations in patients with rhabdoid tumor[J]. Clin Cancer Res, 2011, 17(1): 31-38.
doi: 10.1158/1078-0432.CCR-10-1795 pmid: 21208904 |
| [31] |
Chi SN, Yi JS, Williams PM, et al. Tazemetostat for tumors harboring SMARCB1/SMARCA4 or EZH2 alterations: results from NCI-COG pediatric MATCH APEC1621C[J]. J Natl Cancer Inst, 2023, 115(11): 1355-1363.
doi: 10.1093/jnci/djad085 pmid: 37228094 |
| [32] |
Upadhyaya SA, Campagne O, Billups CA, et al. Phase II study of alisertib as a single agent for treating recurrent or progressive atypical teratoid/rhabdoid tumor[J]. Neuro Oncol, 2023, 25(2): 386-397.
doi: 10.1093/neuonc/noac151 |
| [1] | Rachel Rosen, Osvaldo Borrelli, Christophe Faure, Katja Karrento, Usha Krishnan, Samuel Nurko, Nathalie Rommel, Alan Silverman, Michiel van Wijk, Marc Benninga (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: upper gastrointestinal disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 595-608. |
| [2] | Carlo Di Lorenzo, Miguel Saps, Bruno P. Chumpitazi, Shaman Rajindrajith, Annamaria Staiano, Nikhil Thapar, Miranda van Tilburg, Carlos Velasco-Benítez, Arine Vlieger (Author), Chinese Medical Association Parenteral and Enteral Nutrition Branch Pediatrics Group, The Subspecialty Group of Gastroenterology, The Society of Pediatric, Chinese Medical Association, Gastroenterology Group, Pediatrician Branch, Chinese Medical Doctor Association (Translator). Core interpretation and explanation of Rome Ⅴ diagnostic criteria: lower and biliary disorders of gut-brain interaction in children and adolescents [J]. Journal of Clinical Pediatrics, 2026, 44(7): 609-621. |
| [3] | LI Xufeng, TANG Haoxun, LI Xingjun, ZHANG Lize, GAO Chenqing, ZHAO Shunying, LIU Jianhua. Clinical characteristics, chest CT imaging phenotypes, and their correlation with prognosis in 76 children with Chlamydia pneumoniae pneumonia [J]. Journal of Clinical Pediatrics, 2026, 44(7): 622-627. |
| [4] | WANG Zhen, SHAO Jingbo, ZHANG Na, XIA Min, ZHU Jiashi, DU Chengkan, LI Hong. Factors influencing long-term recurrence in pediatric acute lymphoblastic leukemia patients with low-risk disease at initial diagnosis: a five-year follow-up analysis of 254 cases from a single center [J]. Journal of Clinical Pediatrics, 2026, 44(7): 628-635. |
| [5] | GUO Xuemei, XUE Yao, WANG Yongren, RONG Liucheng, FANG Yongjun, LIN Rufeng. Clinical features and prognosis of childhood acute myeloid leukemia with CBFA2T3::GLIS2 fusion [J]. Journal of Clinical Pediatrics, 2026, 44(7): 636-643. |
| [6] | YANG Lijun, FU Dongxia, CUI Yan, YANG Junmei, ZHANG Liming. Clinical manifestation and genetic analysis of CHARGE syndrome caused by CHD7 gene variation [J]. Journal of Clinical Pediatrics, 2026, 44(7): 644-650. |
| [7] | HU Yan, YANG Fan, LIANG Aimin, MAO Meng. Identification and management of faltering growth in children: insights from the 13th International Conference on Nutrition and Growth [J]. Journal of Clinical Pediatrics, 2026, 44(6): 485-488. |
| [8] | LIU Ziyao, WANG Congying, WANG Hongmao, ZHANG Mingming, XU Yingjie, LAI Jianming, NIU Wenquan, LI Xiaohui. Early differentiation of Kawasaki disease with joint symptoms and systemic juvenile idiopathic arthritis with Kawasaki disease-like symptoms: a single-center retrospective study [J]. Journal of Clinical Pediatrics, 2026, 44(6): 489-498. |
| [9] | LI Yanhua, ZHANG Huanhuan, YANG Jingwei, LIAO Xuelian, SHAO Jingbo, JIAO Yangyang, ZHANG Ting, HUANG Can, JIANG Shayi. Analysis of survival prognosis and related risk factors of pediatric head and neck rhabdomyosarcoma [J]. Journal of Clinical Pediatrics, 2026, 44(6): 518-523. |
| [10] | SHI Yongyuan, YANG Lijuan, LEI Wenting, XIONG Yurong, PAN Shujing, LI Yuelin, ZHANG Jiali, TIAN Maoqiang. Clinical characteristics and prognosis analysis of autoimmune encephalitis with movement disorders in children: A single-center retrospective study [J]. Journal of Clinical Pediatrics, 2026, 44(6): 532-539. |
| [11] | GU Xinjia, ZHENG Zhihui, MEI Lingli, ZHENG Jinxin, LIU Taixiang, ZHU Jihua. Burden of urinary system diseases in children and adolescents in China, 1990-2023 [J]. Journal of Clinical Pediatrics, 2026, 44(6): 546-555. |
| [12] | CHEN Xumei, AIERKEN Aibibai, YUE Xueyan, RU Liang, ZHANG Li. A study on the latent profile analysis of psychological resilience and coping styles of parents of children with asthma and its influencing factors [J]. Journal of Clinical Pediatrics, 2026, 44(6): 556-563. |
| [13] | LUO Zihao, LI Shaojun, REN Peizhen, WANG Yanhong, GENG Gang. Analysis of clinical characteristics of children with pneumonia complicated with plastic bronchitis and establishment and validation of risk prediction model [J]. Journal of Clinical Pediatrics, 2026, 44(6): 564-572. |
| [14] | CHU Weihong, XU Liyan, PENG Shao, LAI Jianming. Lower extremity arterial thrombosis as first clinical manifestation in children's systemic lupus erythematosus complicated with antiphospholipid syndrome: a two-case report [J]. Journal of Clinical Pediatrics, 2026, 44(6): 579-583. |
| [15] | CHEN Liuwang, LIU Pan, XI Rongjuan, ZHANG Xianxia, ZHANG Yi, WEI Xingjiao, SU Min, YANG Yonghong, FU Yangxi. Methylmalonic acidemia with homocystinemia causing subacute combined degeneration of the spinal cord : a case report [J]. Journal of Clinical Pediatrics, 2026, 44(6): 584-588. |
|
||